Advanced Glaucoma Care
Glaucoma
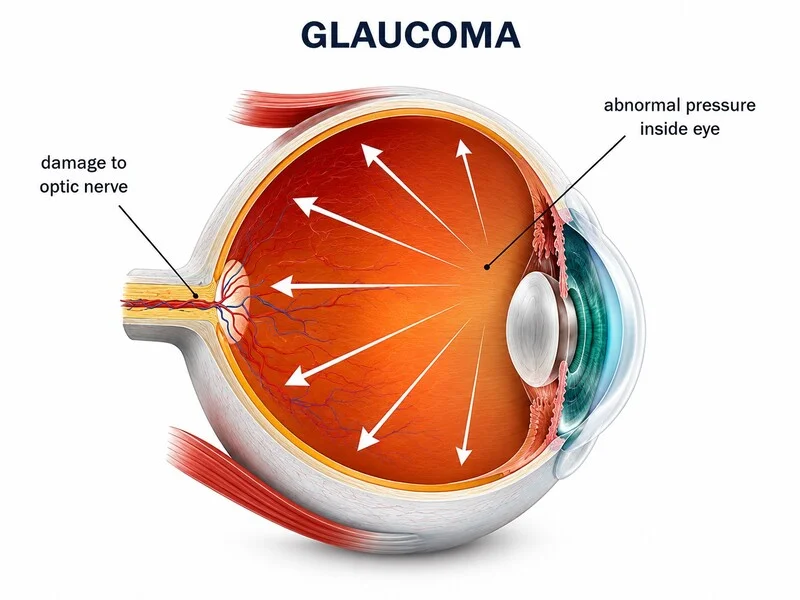
Glaucoma is one of the leading causes of irreversible vision loss worldwide. It affects the optic nerve, the delicate nerve that carries visual signals from the eye to the brain.
Many forms of glaucoma are silent in the early stages. A person may have normal central vision, no pain, and still have progressive optic nerve damage. That is why glaucoma evaluation is not just an eye pressure check — it is a detailed assessment of the optic nerve, eye pressure, visual field and long-term risk of progression.
At Namah, glaucoma care focuses on early detection, advanced imaging, careful pressure assessment, visual field monitoring, counselling and long-term follow-up planning.

What is Glaucoma?
Glaucoma is a group of eye conditions in which the optic nerve gets damaged over time. In majority of the cases, this damage is related to raised eye pressure. However, glaucoma can also occur even when the eye pressure appears to be within the normal range.
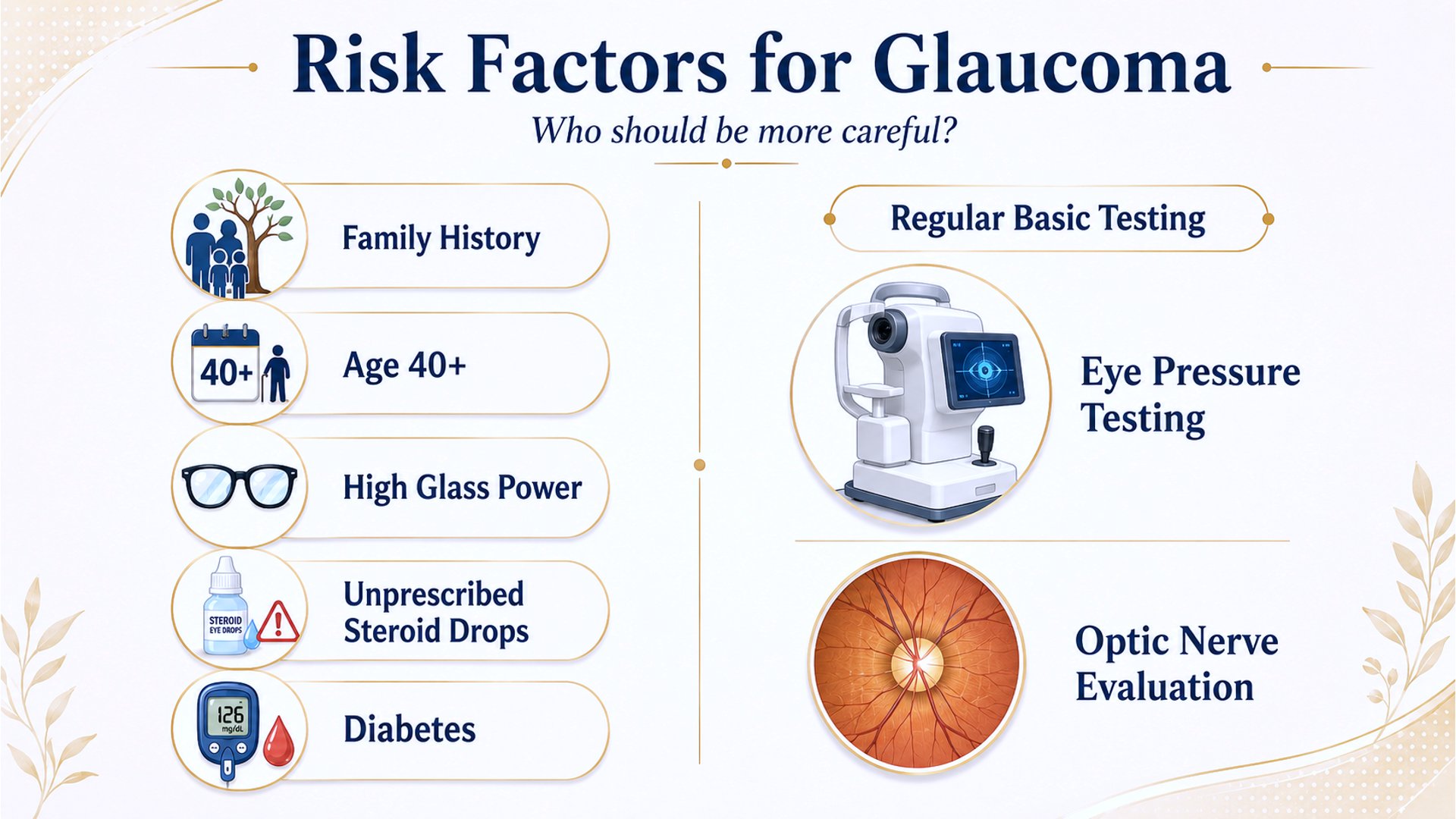
Glaucoma risk is higher in members of the same family and thus, screening of family members is equally important to look for early changes.
The vision loss in glaucoma usually begins from the side vision or peripheral vision. Since central vision may remain good until advanced stages, patients often do not realise that damage is occurring.
Once vision is lost due to glaucoma, it usually cannot be brought back. The aim of treatment thus, is to prevent further damage and preserve remaining vision.
Glaucoma care therefore needs regular monitoring, timely treatment and patient cooperation.
When should you see a glaucoma specialist?
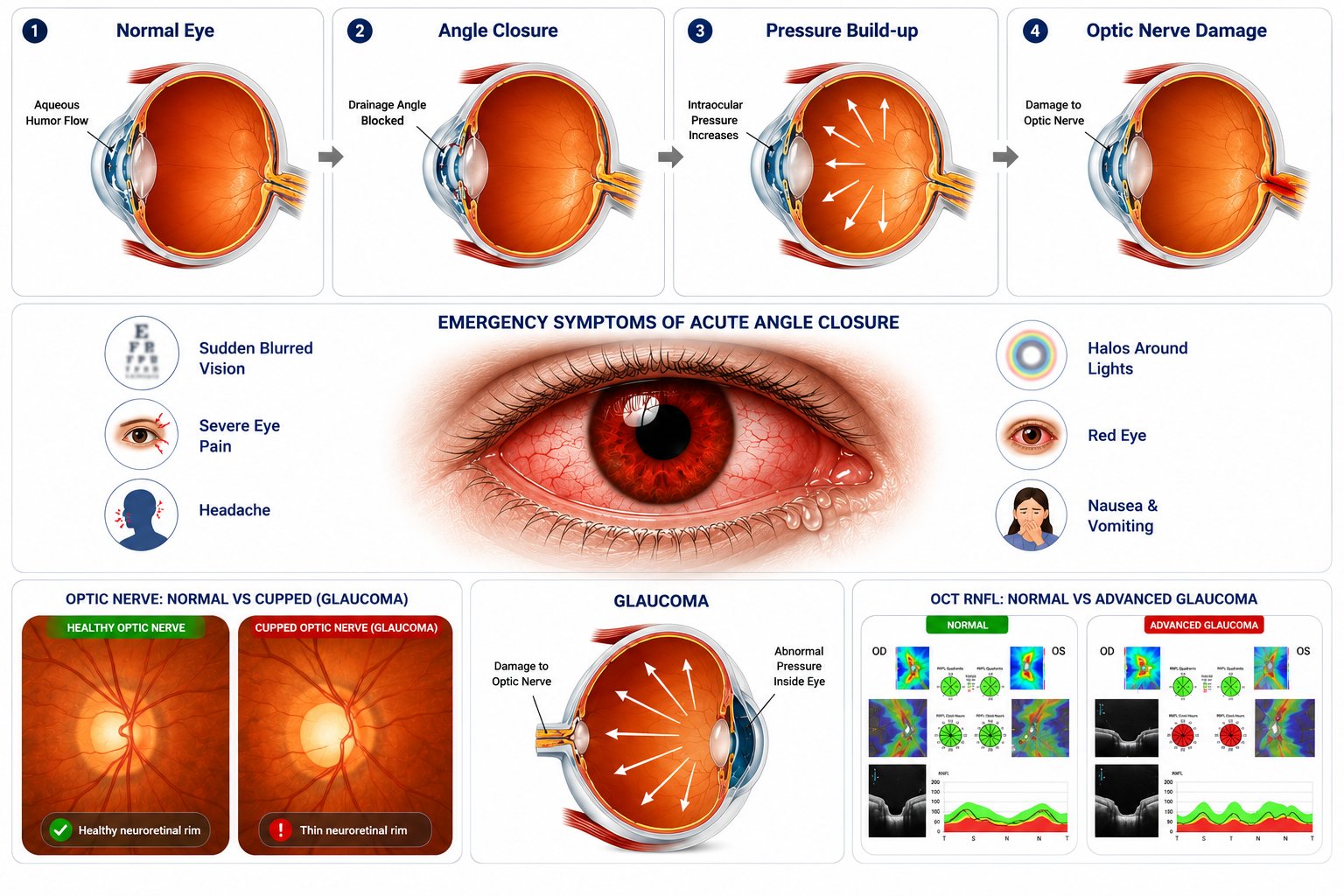
Emergency evaluation is needed in case of sudden eye pain, redness, blurred vision, headache, coloured halos around lights associated with headache, nausea or vomiting.
Patients with gradual loss of side vision, frequent change of glasses, difficulty seeing in dim light or bumping into objects.
Patients with high eye pressure detected during routine eye check-up.
Patients with a family history of glaucoma.
Patients over 40 years of age
Patients with high myopia, previous eye injury, eye inflammation or previous eye surgery.
Patients using steroid eye drops, skin creams, inhalers or tablets for a long period.
Patients with diabetic retinopathy especially in advanced cases
Patients already diagnosed with glaucoma who need long-term follow-up, medication review or progression monitoring
Click on the image to zoom in
What does a glaucoma specialist at Namah evaluate?
From pressure check to vision preservation — a clear glaucoma care pathway.
Symptoms, ocular history, family history and systemic history noted
Vision testing
Refraction and anterior segment evaluation
Eye pressure measurement
Corneal thickness assessment when required
Angle assessment / gonioscopy
Optic nerve evaluation
Dilated retina and optic disc examination when needed
OCT optic nerve and retinal nerve fibre layer and Ganglion Cell complex analysis
Visual field testing
Diagnosis and staging
Target eye pressure planning
Treatment options explained
Drop schedule / procedure plan / follow-up schedule documented.
Glaucoma is not managed by a single pressure reading. Eye pressure, optic nerve structure, visual field function, corneal thickness, angle anatomy and risk factors all need to be interpreted together and monitored at regular intervals to preserve vision.
Namah is well-equipped with advanced diagnostics for glaucoma evaluation and management
Eye Pressure Measurement
Eye pressure, also called intraocular pressure, is one of the most important risk factors in glaucoma. At Namah, Intraocular pressure measurement is done using Non-Contact Tonometry(NCT) in all patients as a screening tool. In cases requiring further evaluation, Goldmann Applanation Tonometry (GAT) is used, which is the gold-standard for IOP evaluation.
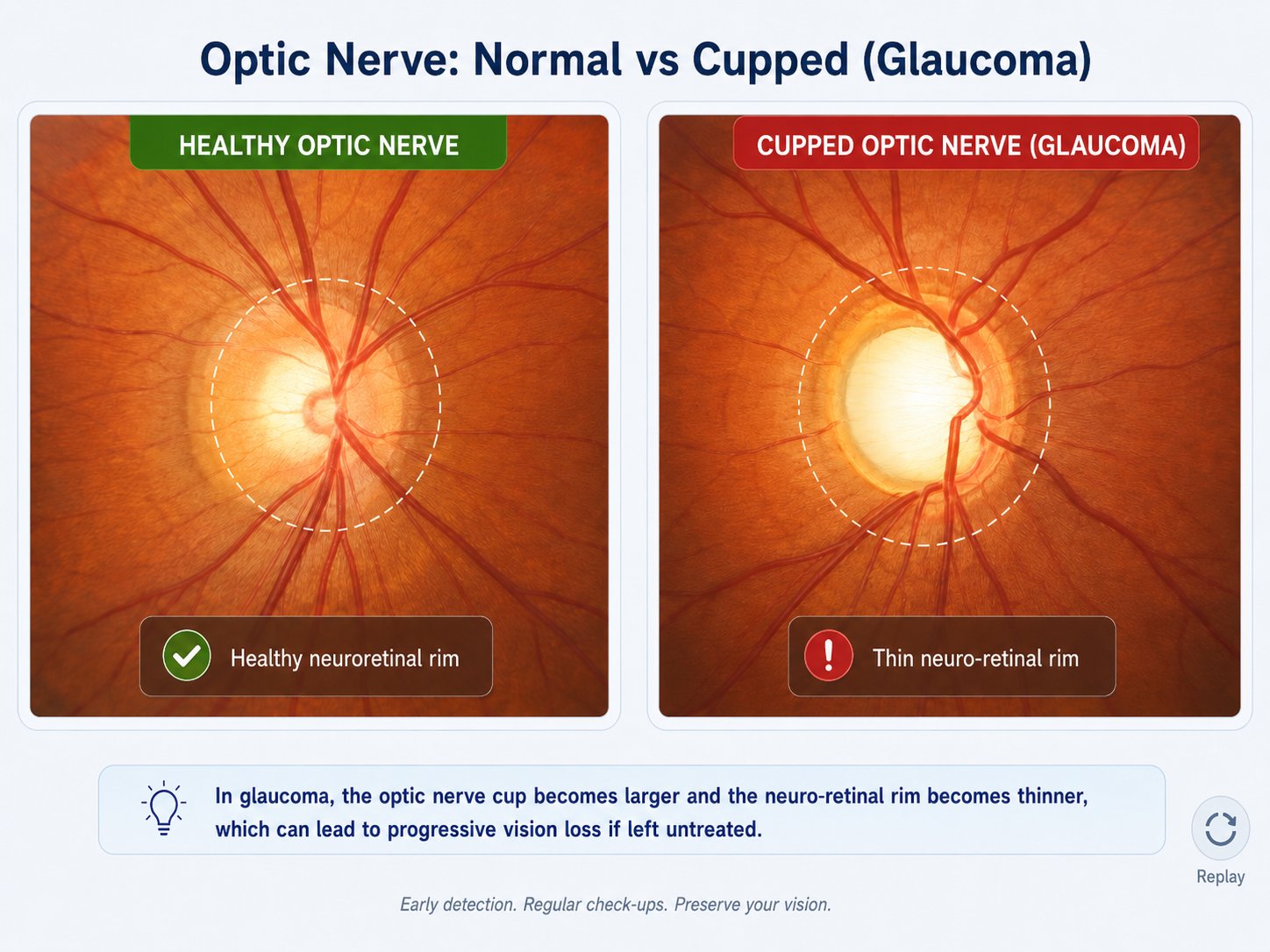
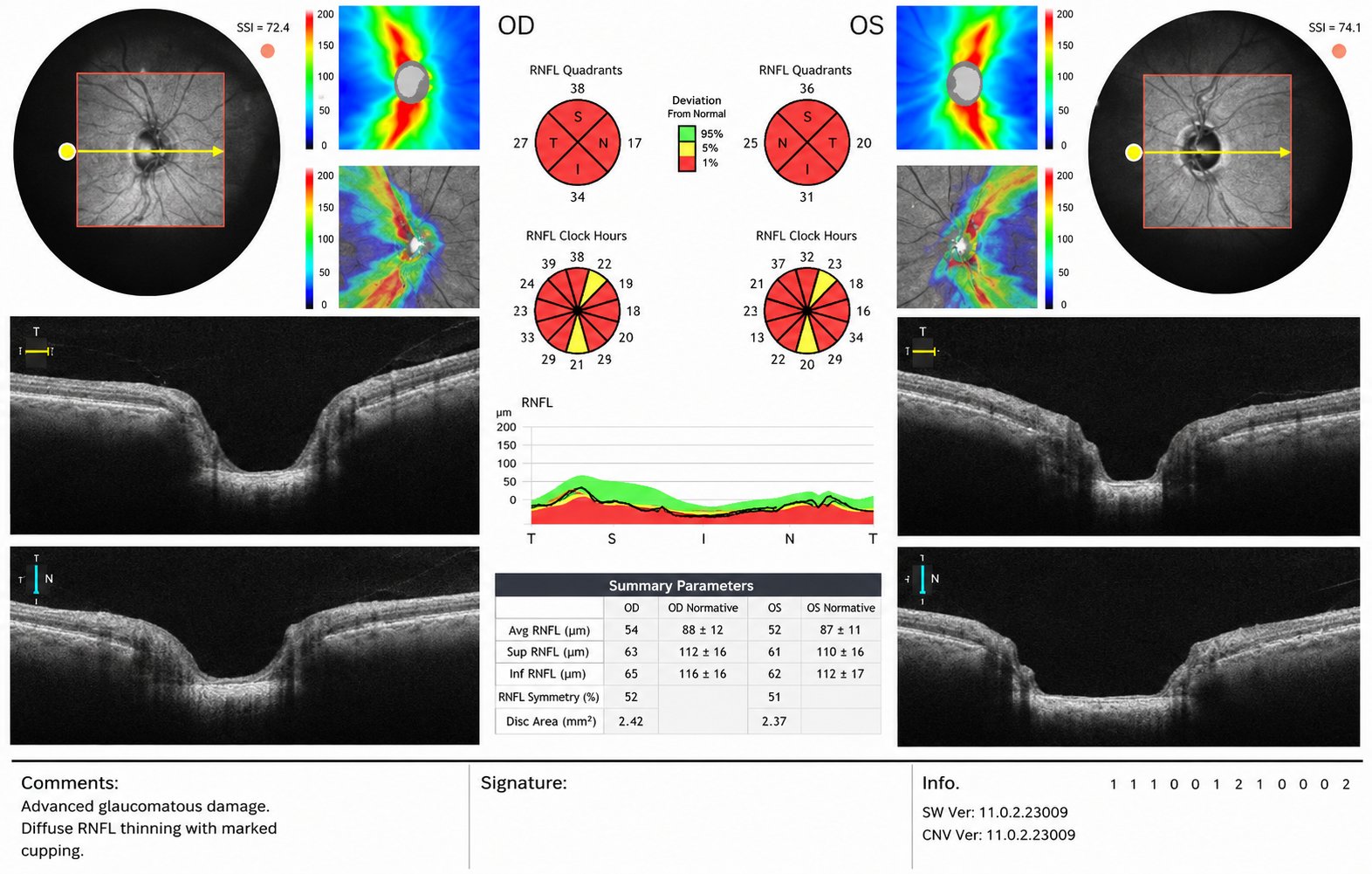
Optic Nerve Evaluation
The optic nerve is carefully examined for signs of glaucomatous damage such as increased cupping, rim thinning, asymmetry between the two eyes, disc hemorrhage or nerve fibre layer loss. This clinical examination remains one of the most important parts of glaucoma diagnosis.
OCT Optic Nerve / RNFL / Ganglion Cell Analysis
Huvitz OCTavius SD-OCT(Spectral domain-Optical coherence tomography) which uses light for speedy and detailed retinal layer imaging, helps in detailed imaging of the optic nerve head, retinal nerve fibre layer and ganglion cell complex. This allows early structural changes to be detected, sometimes even before the patient notices vision loss.
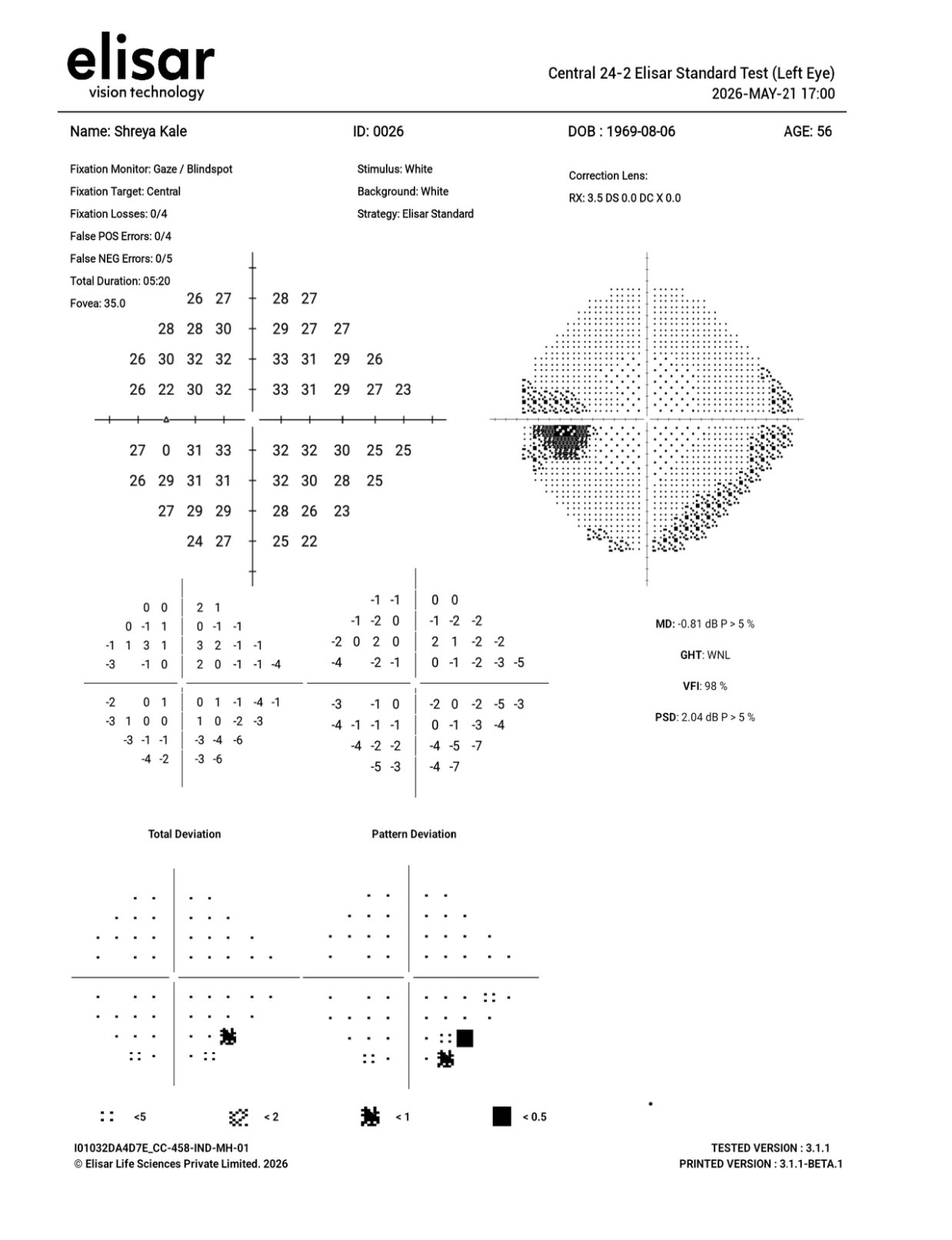
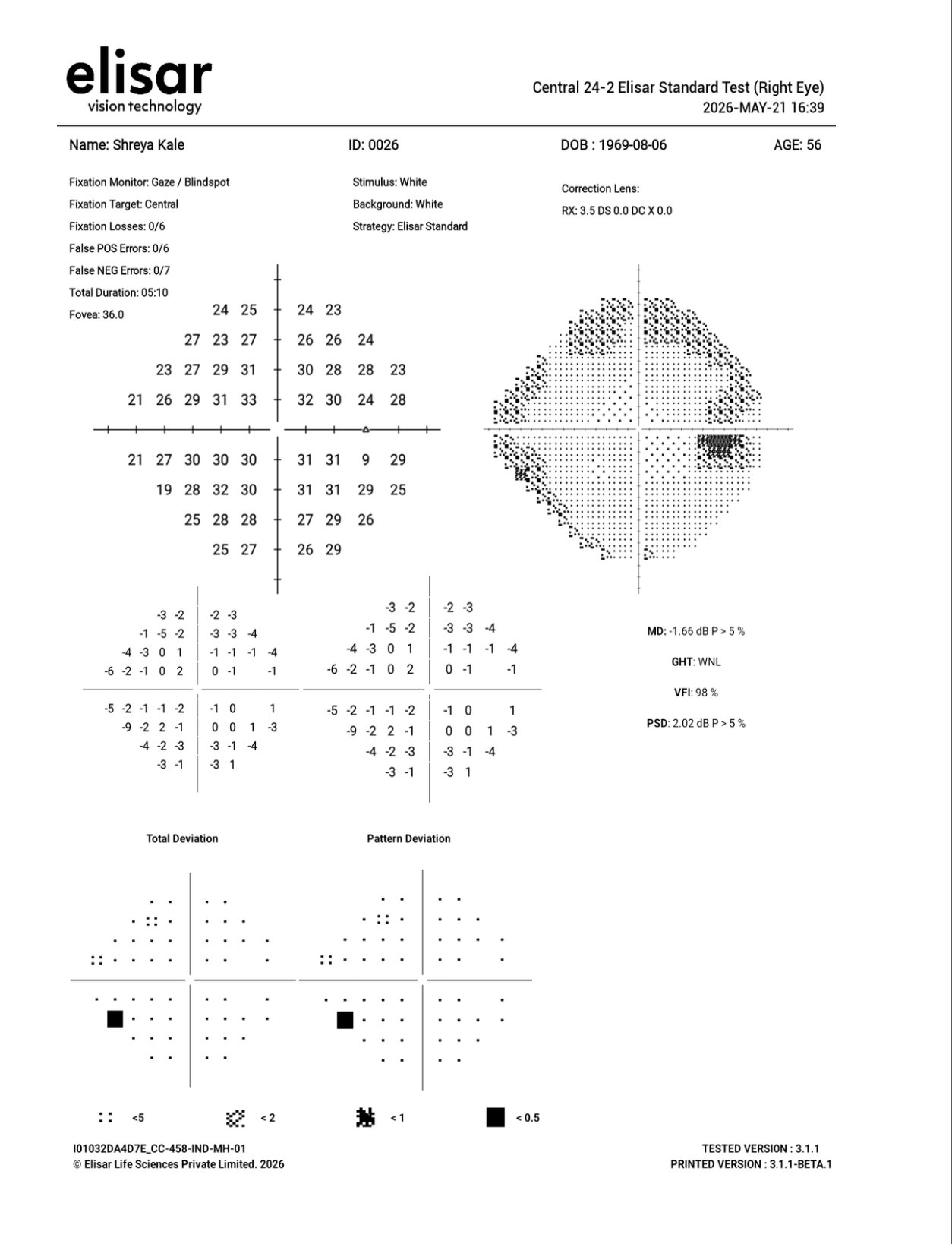
Visual Field Testing
Visual Field Testing using the Elisar AVA (Advanced Vision Analyser), a light-weight, head mounted, portable, virtual reality-based device especially convenient for aging and wheelchair bound patients. Visual field testing helps understand whether the optic nerve damage has started affecting functional vision. It is especially important for staging glaucoma and monitoring progression.
Gonioscopy / Angle Assessment
The drainage angle of the eye is examined to understand whether the glaucoma is open-angle or angle-closure type. This distinction is important because the treatment approach differs.



Click on the image to zoom in
Treatment modalities at Namah
Treatment in glaucoma is customised. The aim is not just to reduce eye pressure, but to reduce it to a safe level for that particular optic nerve. This safe level is called the Target pressure. It depends on the stage of glaucoma, baseline pressure, age, risk factors and whether the disease is progressing.
Anti-Glaucoma Eye Drops
Eye drops are commonly used to lower eye pressure. They may reduce fluid production inside the eye or improve fluid drainage. The drop schedule, timing, side effects and importance of compliance are carefully explained.
Laser Treatment Planning
In selected patients, laser procedures such as laser iridotomy for narrow angles or other glaucoma lasers may be advised depending on the type of glaucoma. The need, timing and expected benefit are explained clearly.
Cataract Surgery in Glaucoma Patients
Cataract surgery in glaucoma patients needs careful planning. In some narrow-angle eyes, cataract removal may help deepen the angle. In advanced glaucoma, pressure control and optic nerve status are carefully considered before surgery.
Surgical Planning for Advanced Glaucoma
Patients with uncontrolled glaucoma despite medicines or progressive optic nerve damage may need glaucoma surgery. Options such as trabeculectomy, glaucoma drainage devices or combined cataract-glaucoma procedures may be discussed depending on the case.
Frequently Asked Questions
I can see clearly. Can I still have glaucoma?
Yes. Glaucoma often affects side vision first. Central vision may remain clear until advanced stages. That is why glaucoma can remain silent for years.
Is glaucoma only about high eye pressure?
No. High eye pressure is an important risk factor, but glaucoma is ultimately a disease of the optic nerve. Some patients have high pressure without glaucoma, while others can have glaucoma even with normal pressure.
Can glaucoma vision loss be reversed?
Usually, no. Vision loss due to glaucoma is generally irreversible. The aim of treatment is to prevent further damage and preserve the remaining vision.
Does glaucoma cause blindness?
Untreated or poorly controlled glaucoma can lead to severe vision loss and blindness. With early diagnosis, regular monitoring and proper treatment, the risk of progression can be significantly reduced.
How often should glaucoma patients follow up?
Follow-up depends on the stage of disease and pressure control. Some stable patients may be reviewed every few months, while advanced or unstable glaucoma may need closer monitoring.
Are glaucoma drops lifelong?
In many patients, glaucoma drops are needed long-term. However, the exact treatment plan depends on the type of glaucoma, pressure control, optic nerve status and progression.
Are glaucoma drops lifelong?
In many patients, glaucoma drops are needed long-term. However, the exact treatment plan depends on the type of glaucoma, pressure control, optic nerve status and progression.
What happens if I forget my drops?
Missing drops repeatedly can allow eye pressure to rise and increase the risk of optic nerve damage. If drops are frequently missed, inform your doctor so that the treatment plan can be adjusted.
Are glaucoma tests painful?
Most glaucoma tests such as eye pressure measurement, OCT and visual field testing are non-invasive. Gonioscopy may cause mild discomfort but is generally well tolerated with numbing drops.
Why do I need visual field testing if OCT is already done?
OCT shows structural damage to the optic nerve and nerve fibre layer. Visual field testing shows how that damage is affecting actual vision. Both tests are important and provide different information.
Can cataract surgery be done in a glaucoma patient?
Yes, cataract surgery can be done in glaucoma patients, but it requires careful planning. The stage of glaucoma, eye pressure, optic nerve status and medications need to be evaluated before surgery.
When is glaucoma an emergency?
Severe eye pain, redness, sudden blurred vision, coloured halos around lights, headache, nausea or vomiting may suggest acute angle-closure glaucoma and needs urgent eye care.