Advanced Neuro-Ophthalmology Care
Neuro-Ophthalmology
At NAMAH Superspeciality Eye Care, neuro-ophthalmology evaluation is focused on detailed clinical examination, imaging-based documentation and timely coordination with neurology or radiology specialities. Some of these conditions may require urgent referrals to avoid life and sight threatening sequelae.
What is Neuro-Ophthalmology?
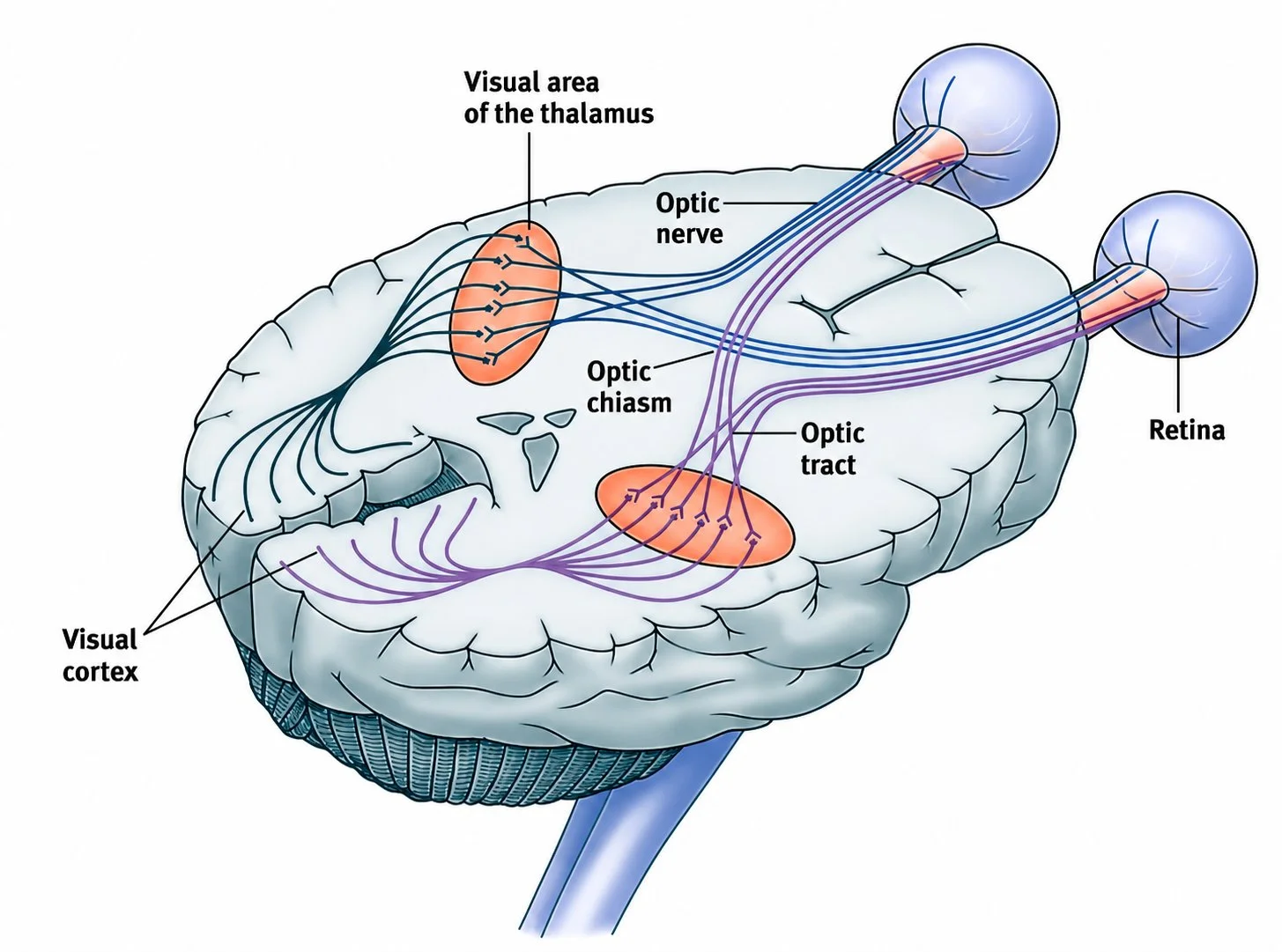
Neuro-ophthalmology deals with eye problems related to the optic nerve, brain, nerves controlling eye movements, pupillary and visual pathways.
The optic nerve carries visual signals from the retina to the brain for processing via a neural network.
Some neuro-ophthalmic conditions are mild and recover with treatment. Others may be warning signs of serious neurological or systemic disease.
That is why careful evaluation is important, especially when symptoms are sudden, unexplained or progressive.
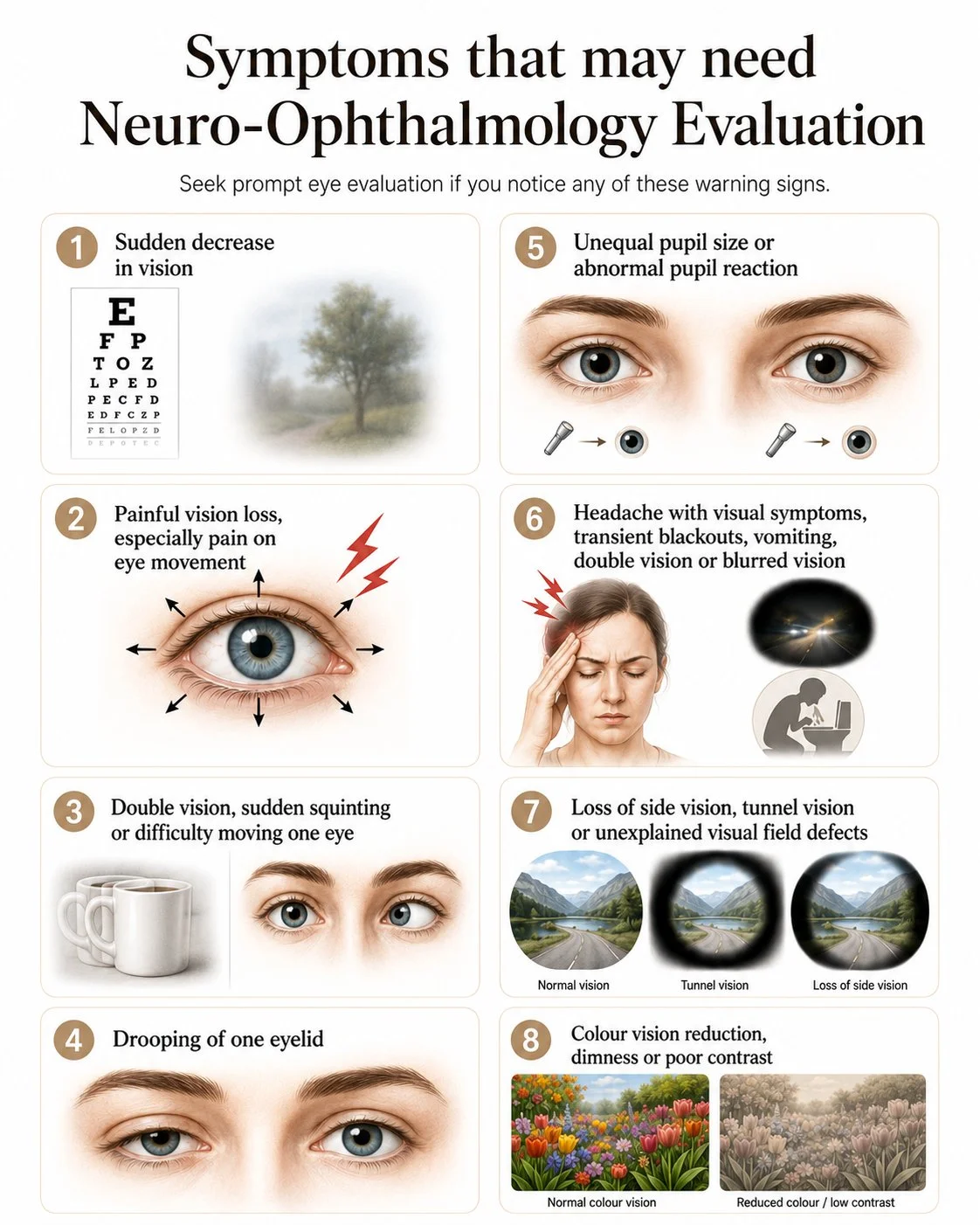
When should you see a Neuro-Ophthalmology specialist?
Sudden decrease/loss in vision- some cases require urgent evaluation and intervention and thus, should not be ignored.
Double vision, sudden squinting or difficulty moving one eye.
Drooping of one eyelid, especially if sudden or associated with double vision.
Unequal pupil size, abnormal pupil reaction or sudden change in pupil appearan
Headache with visual symptoms, transient blackouts, vomiting, double vision or blurred vision.
Loss of side vision, tunnel vision or unexplained visual field defects.
Colour vision reduction, dimness or poor contrast
Patients with neurological disease like stroke, brain tumour, multiple sclerosis needing eye evaluation.
Click on the image to zoom in
What does a Neuro-Ophthalmology specialist at NAMAH evaluate?
From symptom to diagnosis — a structured neuro-ophthalmology care pathway (FLOW CHART)
Symptoms, ocular history, family history and systemic history noted
Symptoms and history
Vision testing
Pupil evaluation, Colour vision testing
Ocular movement assessment, Cranial nerve evaluation
Anterior segment examination
Dilated optic nerve and retina examination
Visual field testing
Counselling, Treatment plan &Referral for MRI
OCT optic nerve / retinal nerve fibre layer / macular ganglion cell analysis
Blood investigations, Neurologist evaluation (depending on the suspected cause)
Specialised Neuro-Ophthalmology diagnostics at NAMAH
At Namah, we use advanced diagnostics to evaluate and to document the progress of the condition.
OCT of Optic Nerve and Retinal nerve fibre layer
OCT helps document and detect changes in the optic nerve and retinal layer thickness. Huvitz OCTavius SD-OCT(Spectral domain-Optical coherence tomography) which uses light for speedy and detailed retinal layer imaging allowing for detection of subtle changes as well as for objectively monitoring disease progression and treatment efficacy.
Visual Field Testing using the Elisar AVA (Advanced Vision Analyser)
A light-weight, head mounted, portable, virtual reality-based device especially convenient for aging and wheelchair bound patients. Visual field testing helps detect missing areas of vision and determining the location of the lesion along the visual pathway.



Click on the image to zoom in
Common Neuro-Ophthalmology Conditions
Optic Neuritis
Inflammation of the optic nerve. It can cause sudden blurred vision, pain on eye movement, colour desaturation and dimness of vision.
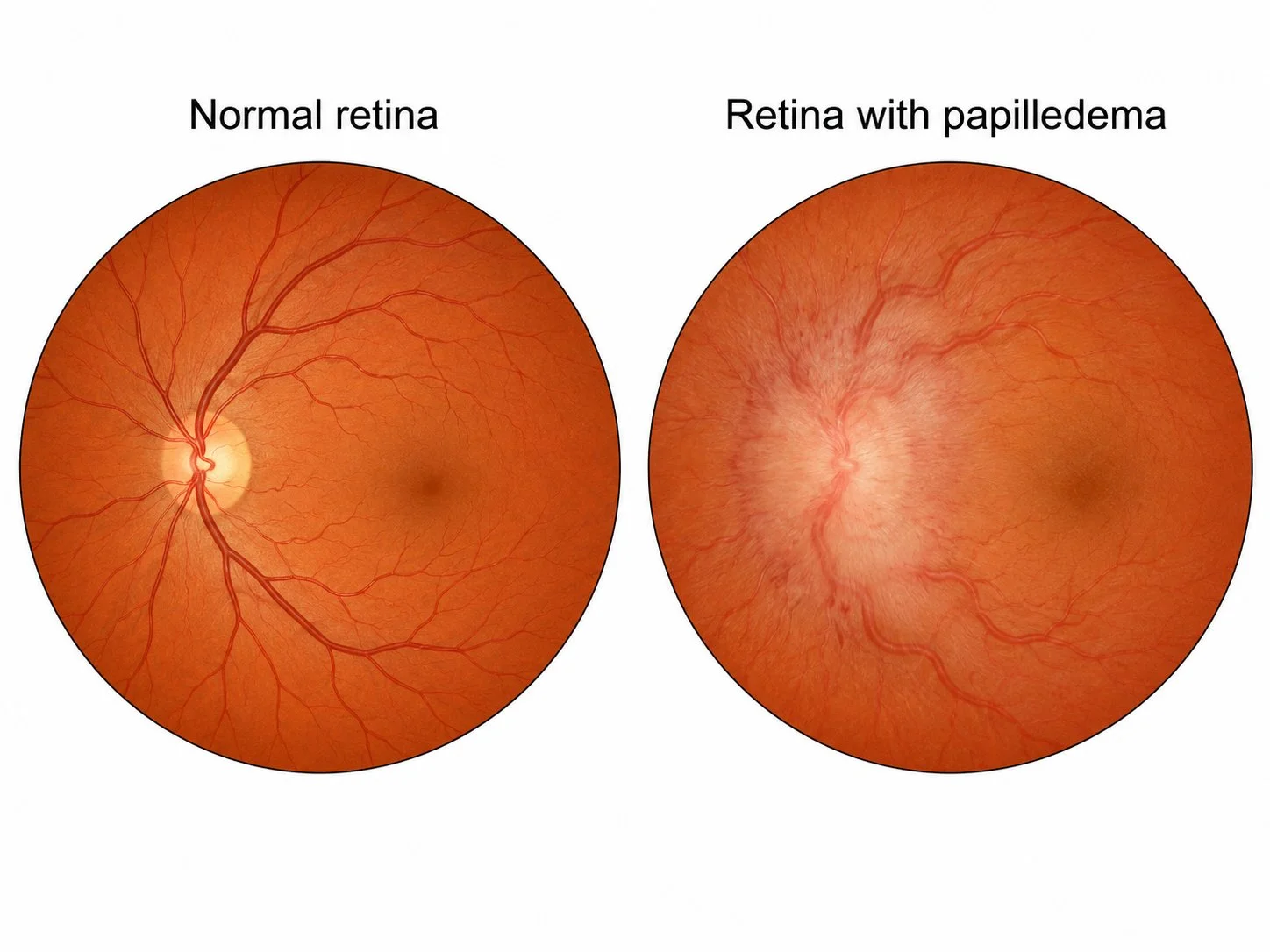
Papilledema
Swelling of the optic nerve due to raised pressure inside the head. Patients may have headache, transient blackouts of vision, vomiting, double vision or blurred vision. It needs urgent evaluation because it may indicate raised intracranial pressure.
Ischemic Optic Neuropathy
Reduced blood supply to the optic nerve, often causing sudden painless vision loss. It is more common in older patients and those with diabetes, hypertension, sleep apnea or vascular risk factor
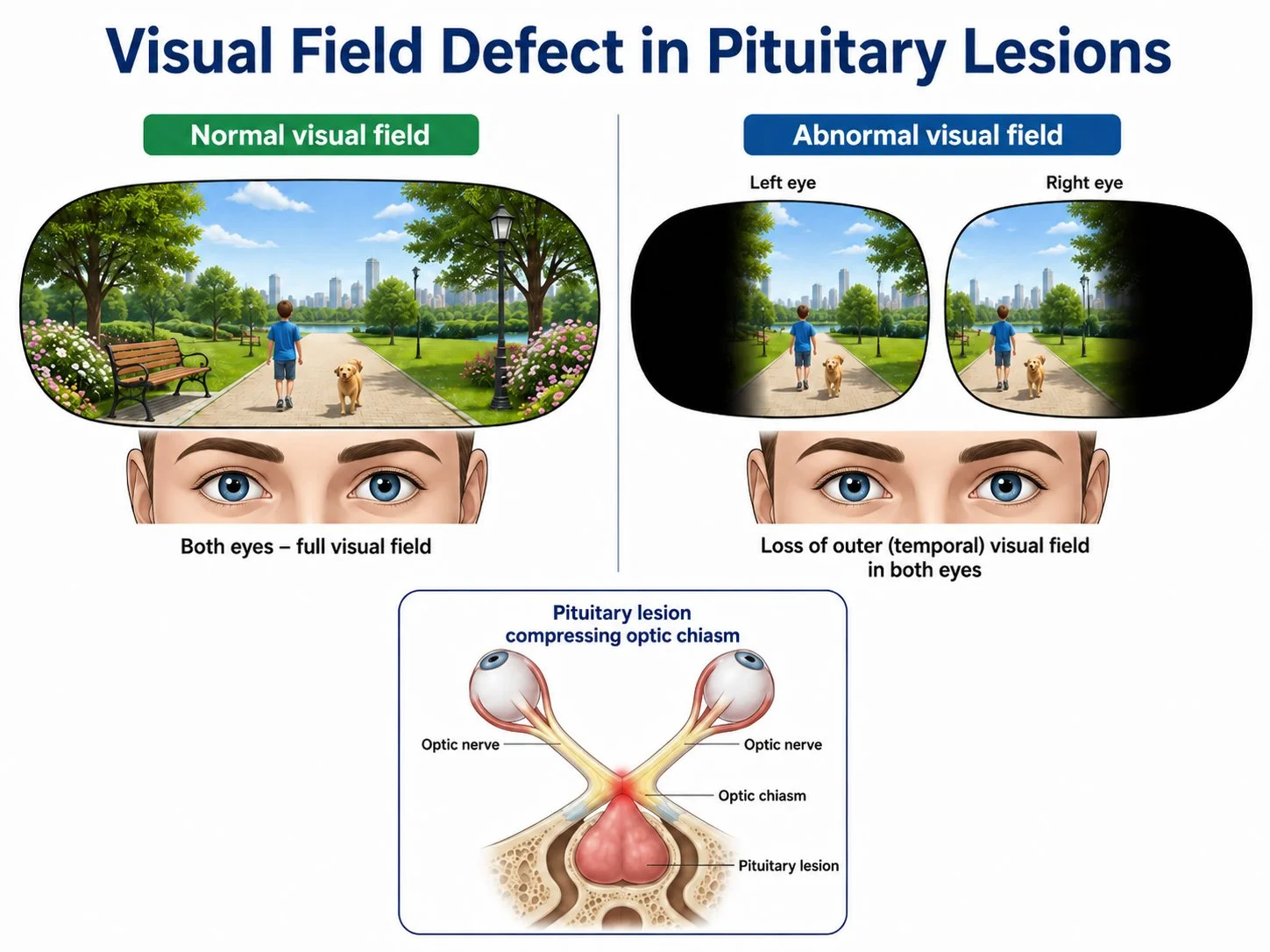
Compressive Optic Neuropathy
Pressure on the optic nerve or visual pathway due to lesions such as pituitary tumours, orbital masses or brain lesions. It may cause gradual vision loss or field defects.
Cranial Nerve Palsy
Weakness of nerves controlling eye movements. It can cause sudden double vision, eye deviation, drooping eyelid or restricted eye movement. Causes may include diabetes, hypertension, aneurysm, inflammation, trauma or brain disease
Ocular Myasthenia Gravis
A condition causing fluctuating drooping of eyelids or double vision. Symptoms may worsen by evening or with fatigue and improve with rest.
Traumatic Optic Neuropathy
Injury to the optic nerve after trauma can lead to sudden reduction in vision. Urgent evaluation is important, especially after head or orbital injury.
Click on the image to zoom in
Frequently Asked Questions
I have sudden vision loss but no redness or pain. Should I still get checked?
Yes. Some serious optic nerve or neurological causes of vision loss may occur even when the eye looks normal from outside. Sudden unexplained vision loss should be evaluated urgently.
What is the optic nerve?
The optic nerve is the nerve that carries visual signals from the eye to the brain. Damage or swelling of the optic nerve can affect vision, colour perception, brightness and visual field.
Is double vision serious?
Sudden double vision can sometimes be due to nerve palsy, diabetes, hypertension, thyroid eye disease, myasthenia or neurological disease. It should be evaluated, especially if it is new, persistent or associated with headache, drooping eyelid or pupil changes.
Does every headache need neuro-ophthalmology evaluation?
No. Most headaches are not due to eye or optic nerve disease. However, headache with blurred vision, transient blackouts, double vision, vomiting, optic nerve swelling or sudden visual symptoms needs proper evaluation.
Why is visual field testing important?
A patient may not notice side vision loss in the early stages. Visual field testing helps detect defects caused by optic nerve disease, glaucoma, pituitary lesions, stroke or brain pathway problems.
Will I need an MRI?
Not every patient needs an MRI. Neuroimaging is advised only when the clinical findings suggest optic nerve or neurological involvement.
Can optic neuritis recover?
Many cases of optic neuritis improve, but the cause and recovery pattern vary. Careful evaluation, systemic correlation and follow-up are important.
Can diabetes cause double vision?
Yes. Diabetes can sometimes affect the nerves controlling eye movement, causing sudden double vision. However, other serious causes also need to be ruled out.
When should I seek emergency care?
Sudden vision loss, sudden double vision, drooping eyelid with pupil change, severe headache with vomiting, transient blackouts of vision, optic nerve swelling or neurological symptoms such as weakness or speech difficulty should be treated as urgent.
At NAMAH, neuro-ophthalmology care is built on detailed clinical examination, optic nerve imaging, visual field assessment, careful counselling and timely multidisciplinary coordination. We understand that neuro-ophthalmic symptoms can be confusing and worrying for patients — our approach is to identify the cause clearly, explain the condition patiently and guide every patient through the right next step.