Advanced Cataract Care
Cataract Services
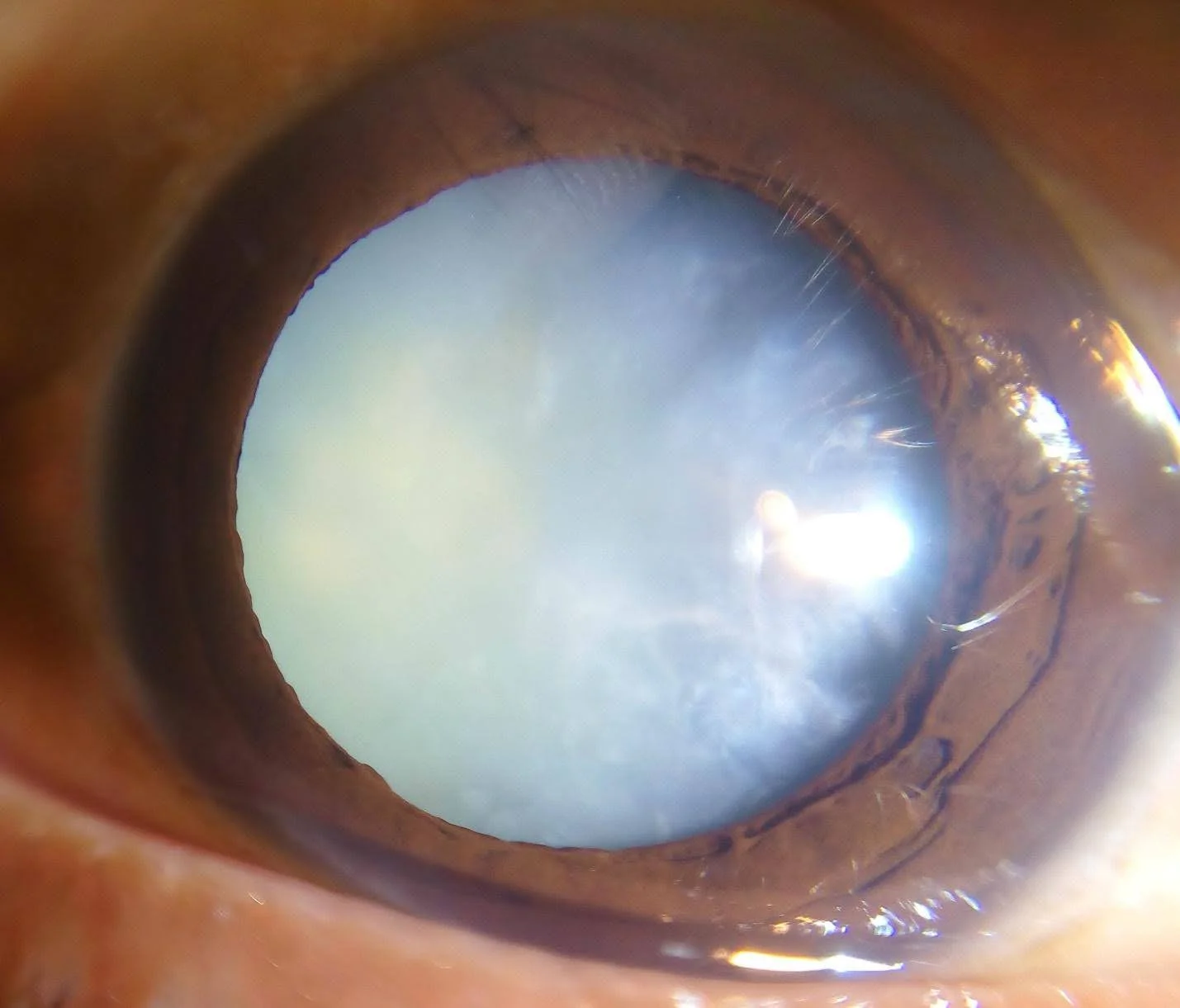
Cataract is one of the most common age-related eye conditions and one of the leading causes of gradual, correctable vision loss. It occurs when the natural clear lens inside the eye becomes cloudy, causing vision to become blurred, dull, hazy or less sharp.
At NAMAH Superspeciality Eye Care, cataract care is not limited to removing the cataract. It begins with detailed evaluation, accurate lens power calculation, personalised intraocular lens selection, careful counselling and precise minimally invasive cataract surgery planning.
What is Cataract?
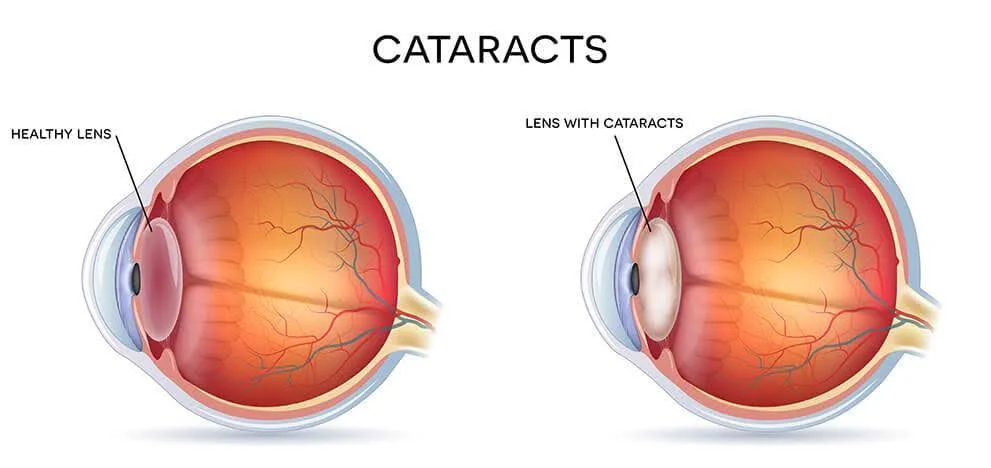
The natural lens of the eye helps focus light clearly on the retina. With age, diabetes, injury, steroid use or other eye conditions, this lens can gradually become cloudy. This clouding is called cataract.
A cataract usually develops slowly. In the early stages, patients may feel that their glasses number is changing frequently or that vision is not as clear as before. As it progresses, daily activities such as reading, driving, using screens, recognising faces or seeing clearly in bright light may become difficult.
Cataract is treatable
The cloudy natural lens is removed and replaced with a clear artificial lens called an intraocular lens, or IOL.
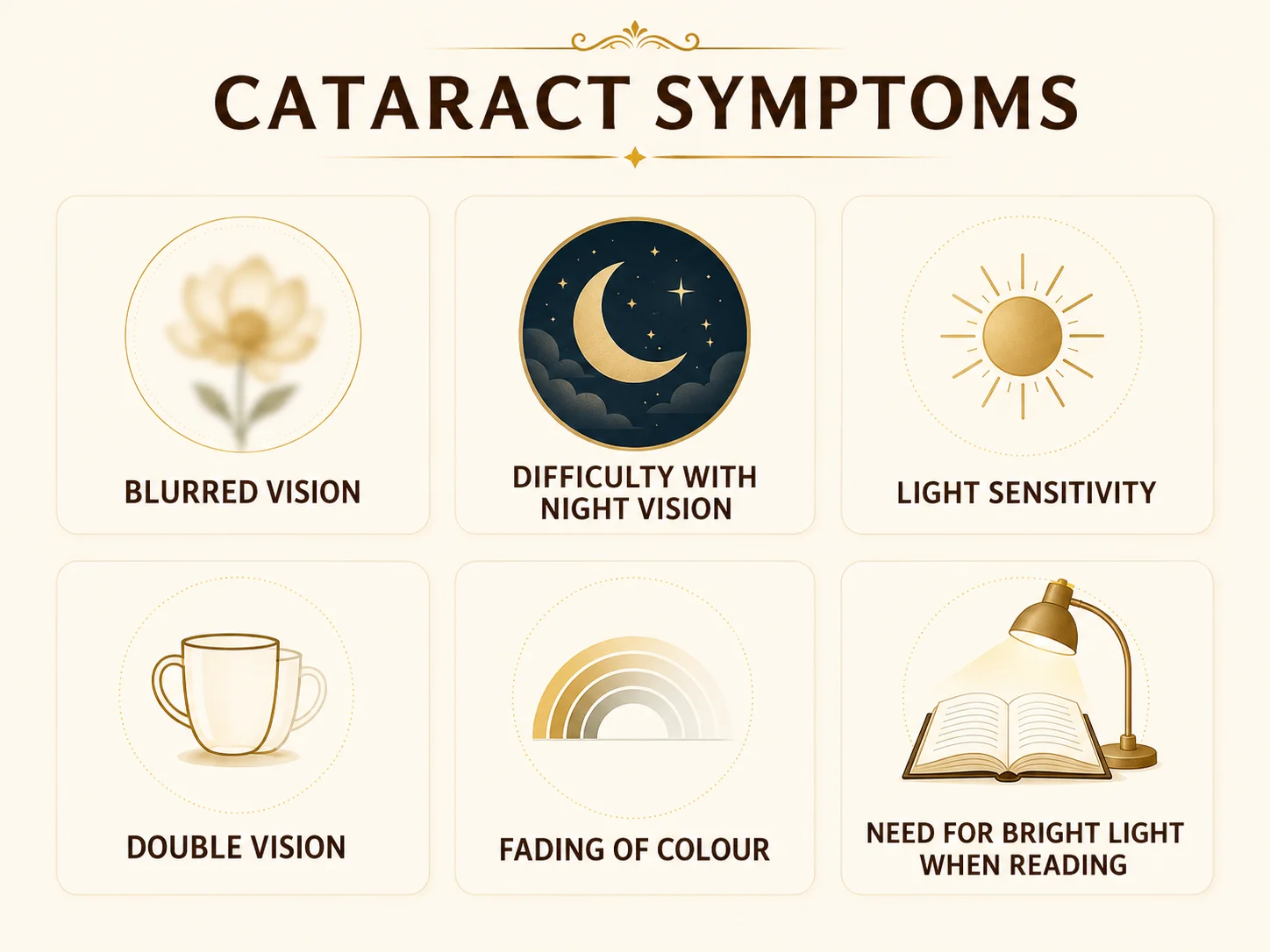
Common Symptoms of Cataract
You should get evaluated for cataract if you notice:
Gradual blurring or haziness of vision
Difficulty seeing clearly while reading, driving or watching television
Glare from headlights, sunlight or bright lights
Halos around lights, especially at night
Faded, dull or yellowish colours
Frequent change in glasses power
Difficulty seeing in dim light
Double or ghost images in one eye
Reduced confidence while driving at night
A feeling that vision is not clear despite changing glasses
Click on the image to zoom in
Cataract usually does not cause redness, pain or sudden vision loss. If vision loss is sudden or associated with pain, flashes, floaters or redness, a detailed eye evaluation is needed to rule out other eye conditions.
When should you see a cataract specialist?
If your vision is affecting reading, driving, screen use or daily work
If you have diabetes, glaucoma, retina disease or previous eye surgery and need cataract planning
If you have been told you have cataract and want to know the right time for surgery
If you have glare or difficulty with night driving
If you are considering premium IOL options and want detailed counselling
If you have cataract in one eye but are unsure whether surgery is needed now
Cataract Evaluation at NAMAH
From blurred vision to clear treatment planning — a structured cataract care pathway.
Step 1
Vision assessment
Step 2
Cataract evaluation
Step 3
Eye pressure check
Step 4
Retinal assessment when required
Step 5
Advanced swept-source biometry for IOL power calculation
Step 6
IOL counselling based on eye health and lifestyle
Step 7
Surgery planning and pre-operative instructions
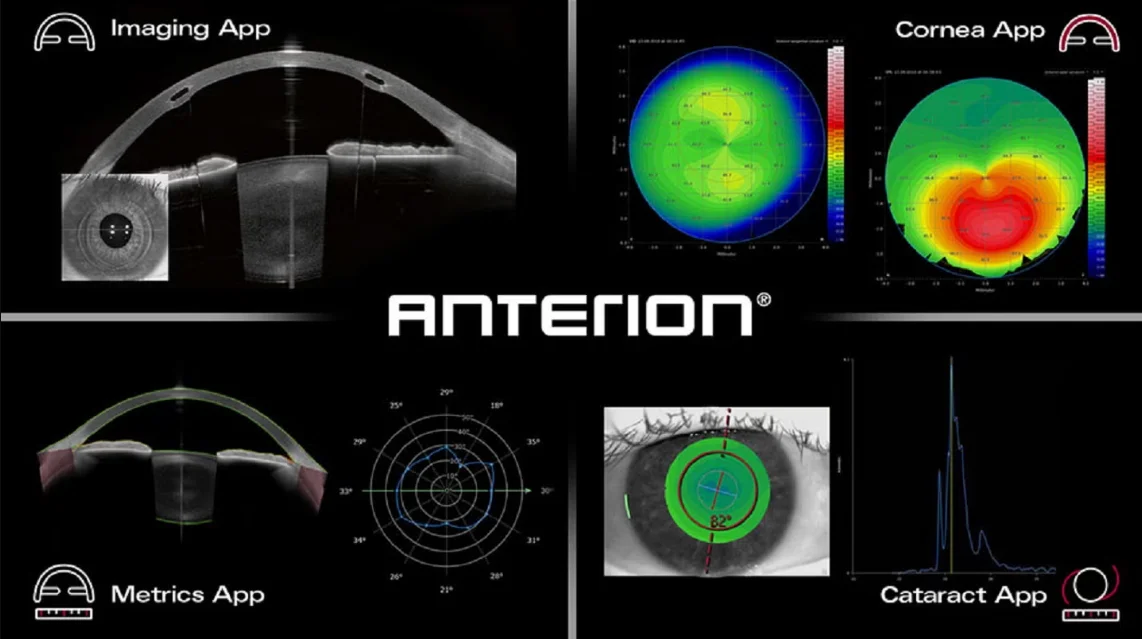
At NAMAH, cataract surgery planning is supported by the ANTERION swept-source OCT biometer — one of the most advanced technologies used for modern IOL power calculation. It captures detailed measurements of the eye, including axial length, corneal curvature, anterior chamber depth and lens thickness, helping the surgeon select the most appropriate intraocular lens power with greater confidence.
This is especially valuable in premium IOL planning, astigmatism correction, short or long eyes, and eyes where accuracy matters even more.
Click on the image to zoom in
At NAMAH, cataract surgery planning is personalised. Every patient’s eye structure, cataract type, retina status, corneal health, astigmatism, lifestyle requirements and visual expectations are considered before deciding the surgical plan and IOL type.

Click on the image to zoom in
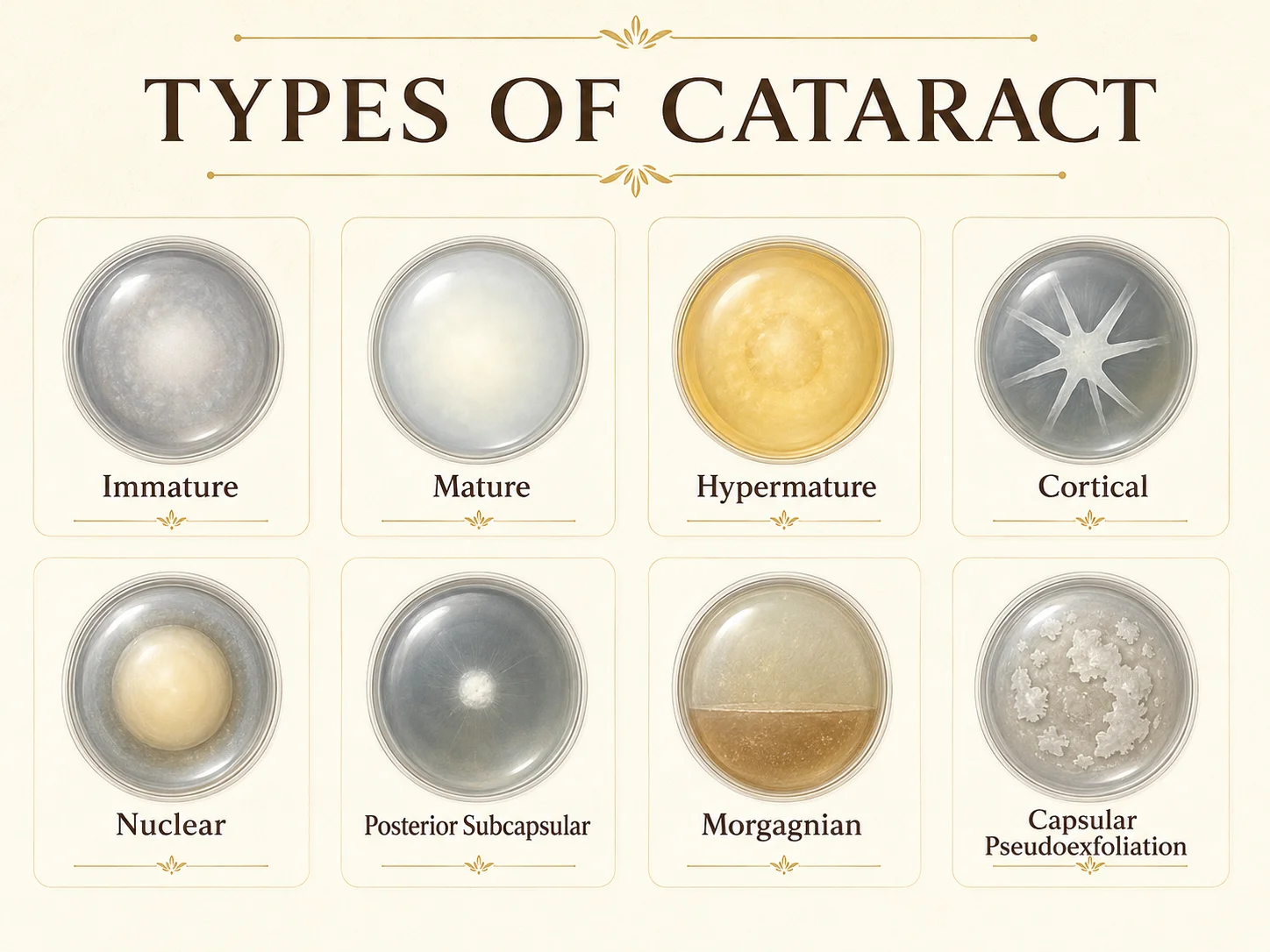
Types of Cataract
01
Nuclear cataract
This is the common age-related cataract that affects the central part of the lens. Patients may notice gradual blurring, yellowing of vision, reduced contrast and changes in glasses number.
02
Cortical cataract
This type affects the outer layers of the lens. It may cause glare, scattered light and difficulty in bright illumination.
03
Posterior subcapsular cataract
This cataract forms near the back surface of the lens. It can cause significant glare, difficulty reading and reduced vision even when the cataract appears small. It may be seen in younger patients, diabetics or patients with steroid exposure.
04
Mature cataract
In advanced cataract, the lens becomes significantly cloudy and vision may be severely reduced. Surgery may be more complex and should be planned carefully.
05
Cataract with other eye conditions
Cataract may coexist with glaucoma, diabetic retinopathy, macular disease, corneal problems or dry eye. These cases need additional evaluation before surgery so that visual expectations and surgical planning are realistic.
Click on the image to zoom in
Cataract Surgery at NAMAH
Cataract surgery at NAMAH is performed using topical, minimally invasive phacoemulsification
In phacoemulsification, the cloudy natural lens is broken into tiny fragments using ultrasonic energy and removed through a small incision. A clear foldable intraocular lens is then implanted inside the eye.
The procedure is usually performed with numbing eye drops, without the need for routine injection anesthesia in most cases. Because the incision is very small, healing is usually faster and stitches are often not required.

Click on the image to zoom in
Oertli OS4 phacoemulsification platform
At NAMAH, cataract surgery is performed using the Oertli OS4 surgical platform.
The Oertli OS4 is an advanced ophthalmic surgical platform used for cataract and vitreoretinal surgery. In cataract surgery, it supports controlled phacoemulsification, stable fluidics and efficient lens removal. This helps the surgeon work with precision inside the eye while maintaining a stable surgical environment.
For patients, this means that cataract surgery is planned with modern technology, controlled energy delivery and careful intraoperative stability.
The machine is important, but the outcome depends on the complete process — pre-operative evaluation, surgical judgement, IOL selection, sterile technique and post-operative follow-up.
Key Features of Cataract Surgery at NAMAH
Topical anesthesia using numbing eye drops in suitable cases
Minimally invasive small-incision phacoemulsification
Foldable IOL implantation
Personalised IOL power calculation
Astigmatism and lifestyle-based lens counselling
Retina and glaucoma evaluation when required
Modular OT-based sterile surgical care
Clear post-operative instructions and follow-up planning
Cataract surgery in patients with diabetes
Patients with diabetes need careful retinal evaluation before cataract surgery. Diabetic retinopathy or diabetic macular edema may affect vision even after technically successful cataract surgery.
At NAMAH, diabetic patients may undergo dilated retinal examination and OCT-based macular evaluation when indicated. If diabetic retina disease is present, treatment and follow-up are planned accordingly.
Cataract surgery in glaucoma patients
Cataract surgery in glaucoma patients needs special planning. Eye pressure, optic nerve status, angle anatomy, visual field status and current glaucoma medications are reviewed before surgery.
In some narrow-angle eyes, cataract surgery may help deepen the angle. In advanced glaucoma, surgery is planned with extra caution and realistic visual expectations.
Cataract surgery in retinal disease patients
If a patient has age-related macular degeneration, diabetic macular edema, previous retinal detachment, macular hole, epiretinal membrane or other retinal conditions, the retina status is evaluated before surgery.
This helps in explaining expected visual recovery and planning any retina treatment or monitoring that may be required.
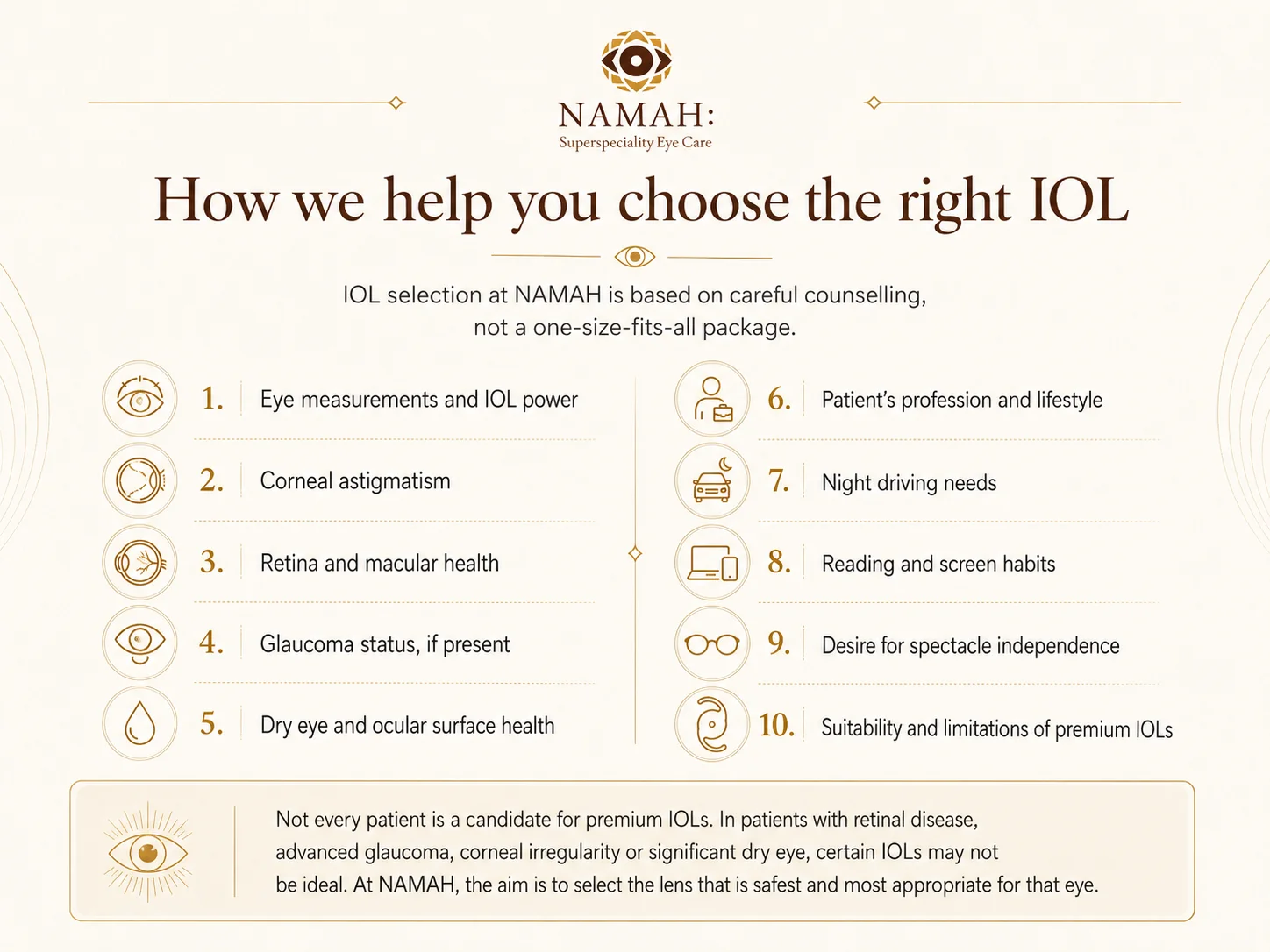
Intraocular Lens Options
During cataract surgery, the cloudy natural lens is replaced with an artificial intraocular lens, commonly called an IOL. The choice of IOL is an important part of cataract planning. The best IOL is not the same for every patient. It depends on eye measurements, corneal astigmatism, retina health, glaucoma status, dry eye, lifestyle, reading needs, night driving habits and patient expectations.
01
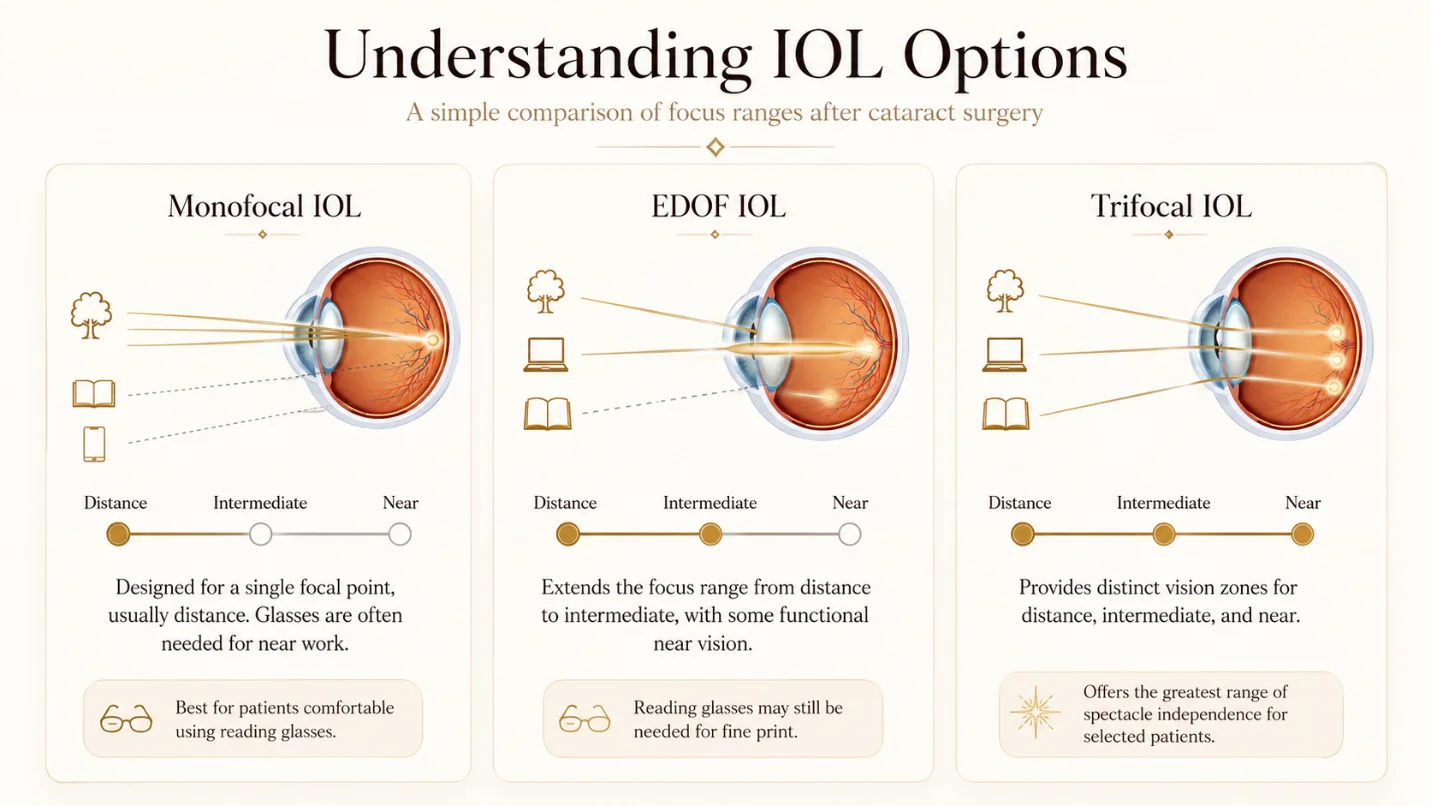
Monofocal IOL
A monofocal IOL is designed to provide clear vision at one main distance, usually distance vision. Most patients may still need glasses for reading or near work,
Best suited for
Patients who want reliable distance clarity and are comfortable using reading glasses.
02
Toric IOL
A toric IOL corrects cataract along with significant corneal astigmatism. It helps improve unaided distance vision in patients who have suitable astigmatism.
Best suited for
Patients with regular corneal astigmatism who want better distance vision without depending heavily on cylindrical glasses.
03
Multifocal / Trifocal IOL
These lenses are designed to reduce dependence on glasses for more than one distance, such as distance, intermediate and near vision. They may not be suitable for every eye and can sometimes be associated with halos, glare or contrast sensitivity issues.
Best suited for
Carefully selected patients with healthy retina, healthy cornea and realistic expectations.
04
Extended Depth of Focus / EDOF IOL
EDOF lenses are designed to provide an extended range of vision, especially distance and intermediate vision, with reduced dependence on glasses for many routine activities. Reading glasses may still be needed for fine near work.
Best suited for
Patients who want a broader range of functional vision and may prefer fewer visual disturbances compared with some multifocal designs.
05
Monofocal-plus / Enhanced monofocal IOL
These lenses aim to provide good distance vision with some improvement in intermediate functional vision compared with a standard monofocal lens. Near glasses are usually still required.
Best suited for
Patients who want quality distance vision with some functional intermediate benefit.
Click on the image to zoom in
Patient Journey for Cataract Surgery at NAMAH
Step 1
Diagnosis
The cataract is assessed clinically and correlated with the patient’s symptoms and visual needs.
Step 2
Eye measurements
Biometry and eye measurements are performed to calculate the IOL power.
Step 3
Eye health assessment
The cornea, retina, optic nerve and ocular surface are evaluated when required.
Step 4
IOL counselling
Different lens options are explained in a simple, practical way based on the patient’s eye health and lifestyle.
Step 5
Surgery planning
The surgical plan, anesthesia, precautions, medications and follow-up schedule are explained.
Step 6
Cataract surgery
Topical minimally invasive phacoemulsification with foldable IOL implantation is performed using the Oertli OS4 platform.
Step 7
Follow-up and recovery
Post-operative medicines, precautions and follow-up visits are explained clearly. Vision recovery is monitored and glasses are prescribed if needed.
Frequently Asked Questions
Is cataract surgery painful?
Most cataract surgeries are performed using numbing eye drops. Patients may feel mild pressure, water flow or light, but significant pain is uncommon.
How long does cataract surgery take?
The actual surgery is usually short, but the total clinic/OT time is longer because of preparation, dilation, cleaning, surgery and post-operative instructions.
Will I need stitches?
In modern phacoemulsification, the incision is very small and usually does not require stitches. However, this depends on the surgical situation.
Is cataract surgery done by laser?
The most common modern cataract surgery is phacoemulsification, where ultrasound energy is used to break and remove the cataract. Laser-assisted cataract surgery is a separate technology and is not required in every case.
Will I need glasses after cataract surgery?
This depends on the IOL selected, astigmatism, healing, eye condition and visual needs. Some patients need glasses only for near work, while others may need glasses for certain tasks even after surgery.
Which IOL is best?
There is no single best IOL for everyone. The right IOL depends on your eye measurements, retina health, cornea, glaucoma status, lifestyle and expectations.
Are premium IOLs suitable for everyone?
No. Multifocal, trifocal or EDOF lenses may not be suitable in patients with certain retinal, corneal, glaucoma or ocular surface conditions. Suitability must be assessed carefully.
Can cataract come back after surgery?
The cataract itself does not come back because the cloudy natural lens is removed. However, the thin capsule behind the IOL may become cloudy in some patients over time. This is called posterior capsular opacification and can usually be treated with a quick laser procedure if needed.
When should cataract surgery be done?
Cataract surgery is usually advised when cataract starts affecting daily activities, quality of vision or safety. In some cases, surgery may be advised earlier if the cataract is affecting retinal examination, glaucoma management or eye pressure.
Can both eyes be operated on the same day?
In many practices, cataract surgery is commonly performed one eye at a time. The timing of the second eye is planned depending on visual needs, recovery and surgeon preference.
How soon can I return to routine activities?
Most patients resume light routine activities soon after surgery, but eye rubbing, water exposure, dust, heavy lifting and strenuous activity should be avoided as advised.
Is cataract surgery safe in elderly patients?
Cataract surgery is commonly performed in elderly patients. Fitness, systemic conditions, medications and eye health are reviewed before surgery.
At NAMAH, cataract care goes beyond removing a cloudy lens. Our approach combines detailed examination, accurate diagnostics, personalised IOL counselling, minimally invasive phacoemulsification and structured follow-up. We understand that cataract surgery is both a medical procedure and a life-quality decision — and we guide every patient through it with clarity, precision and care.