Advanced Refractive Surgery & Keratoconus Care
Refractive Surgery & Keratoconus
Refractive Vision Correction at NAMAH:
Refractive vision correction is not one single procedure. It includes multiple options such as laser vision correction, phakic intraocular lenses and selected lens-based procedures. The right choice depends on a detailed understanding of the eye – not just the glasses number.
At NAMAH Superspeciality Eye Care, refractive surgery planning begins with a structured suitability assessment. We evaluate the spectacle power, corneal thickness, corneal shape, anterior chamber depth, dry eye status, retina health and lifestyle needs before recommending any procedure.

Click on the image to zoom in
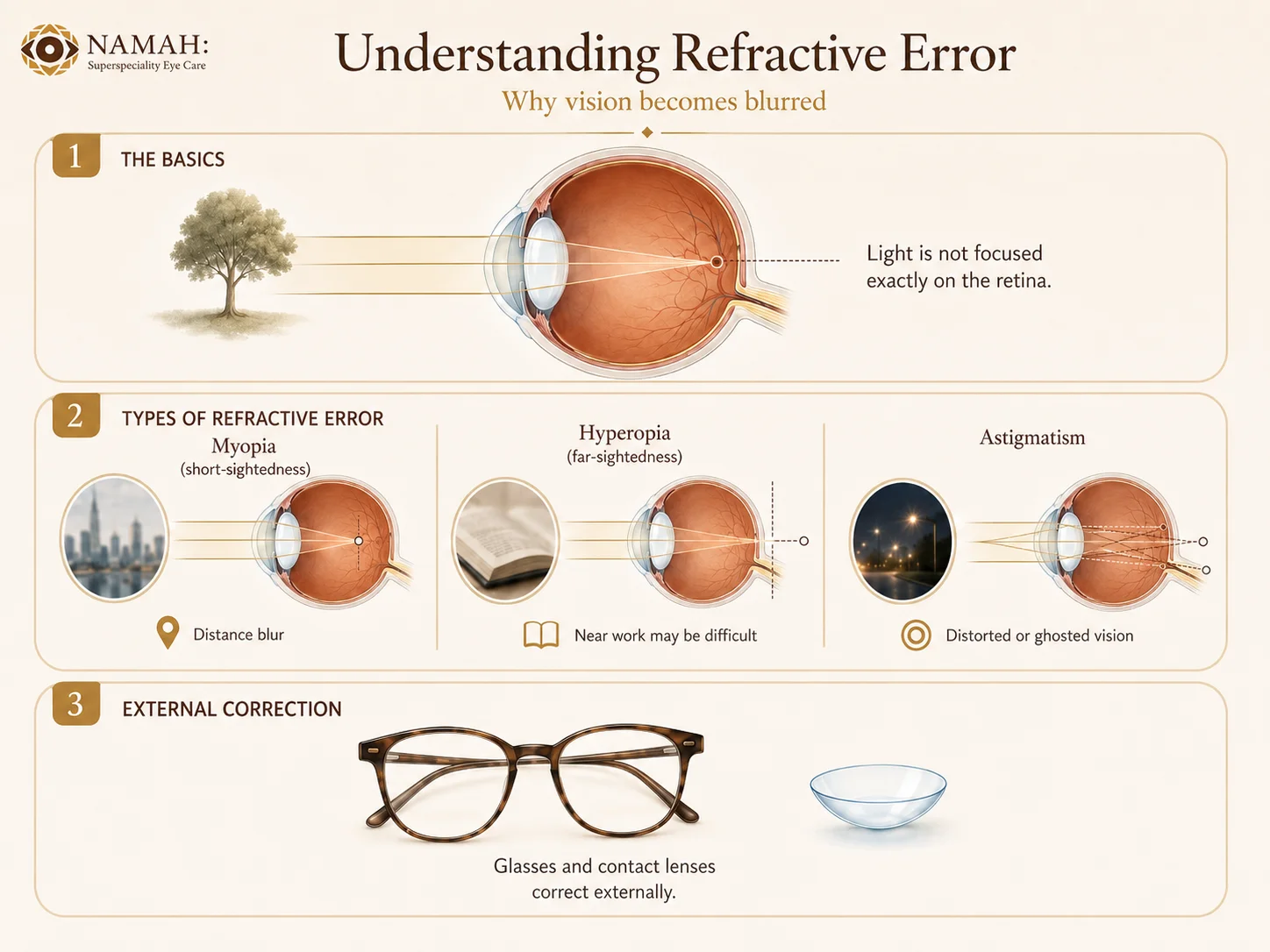
What is Refractive Error?
A refractive error occurs when the eye does not focus light precisely on the retina. This can cause blurred vision and the need for glasses or contact lenses.
Myopia / short-sightedness
Distant objects appear blurred while near vision is usually clearer.
Hyperopia / far-sightedness
Near work may be difficult and some patients may also experience distance blur or eye strain.
Astigmatism
the cornea or lens has unequal curvature, causing distorted or ghosted vision.
Glasses and contact lenses correct refractive error externally. Refractive surgery aims to reduce dependence on glasses or contact lenses by changing the focusing system of the eye, either at the cornea or by placing a corrective lens inside the eye.
Refractive surgery is elective. That makes careful screening, honest counselling and realistic expectations extremely important.
Who Should Consider a Refractive Surgery Evaluation?
A refractive surgery evaluation may be useful for:
Adults with stable glasses power
Patients wanting reduced dependence on glasses or contact lenses
High myopia patients who may not be ideal for laser procedures
Patients with thin corneas or borderline corneal thickness
Patients intolerant to contact lenses
Patients considering ICL or IPCL
Patients previously told they are not suitable for LASIK
Patients with suspected keratoconus or abnormal corneal maps
Patients with family history of keratoconus
Patients with frequent change in cylindrical power
Patients who rub their eyes frequently or have allergy
Patients wanting detailed counselling before choosing a refractive procedure
Refractive Surgery Options: An Overview
The main categories of refractive correction include corneal laser procedures and lens-based procedures. Each has different eligibility requirements, advantages and limitations.
LASIK
Reshapes the cornea using laser to reduce glasses power.
Needs adequate corneal thickness, stable power and normal corneal tomography. Not ideal in keratoconus, suspicious corneas or significant dry eye.
SMILE
A flapless laser vision correction procedure used mainly for myopia and myopic astigmatism.
Suitability depends on power, corneal parameters and surgeon assessment. It is performed at specialised laser centres.
PRK / Surface Ablation
Reshapes the surface of the cornea without creating a flap.
May be considered in selected patients, including some with thinner corneas, but healing and discomfort profile differs from LASIK/SMILE.
ICL / IPCL
Places an implantable lens inside the eye while preserving the natural crystalline lens.
Useful in selected patients with higher powers, thin corneas or patients unsuitable for corneal laser correction. Requires detailed internal eye measurements.
At NAMAH, phakic IOL evaluation and surgery are offered in-house for suitable patients. Laser procedures such as LASIK, SMILE and PRK are explained for patient education and may be advised at a specialised laser refractive surgery centre when appropriate.
Phakic IOLs: ICL and IPCL
Phakic IOLs are implantable lenses placed inside the eye while preserving the natural crystalline lens. Unlike laser vision correction, they do not remove corneal tissue. This makes them an important option for selected patients with higher spectacle power, thin corneas or those who are not ideal candidates for corneal laser procedures.
ICL and IPCL are not cosmetic contact lenses. They are intraocular implants and therefore require detailed pre-operative measurements, surgical planning, sterile surgery and follow-up.
Click on the image to zoom in
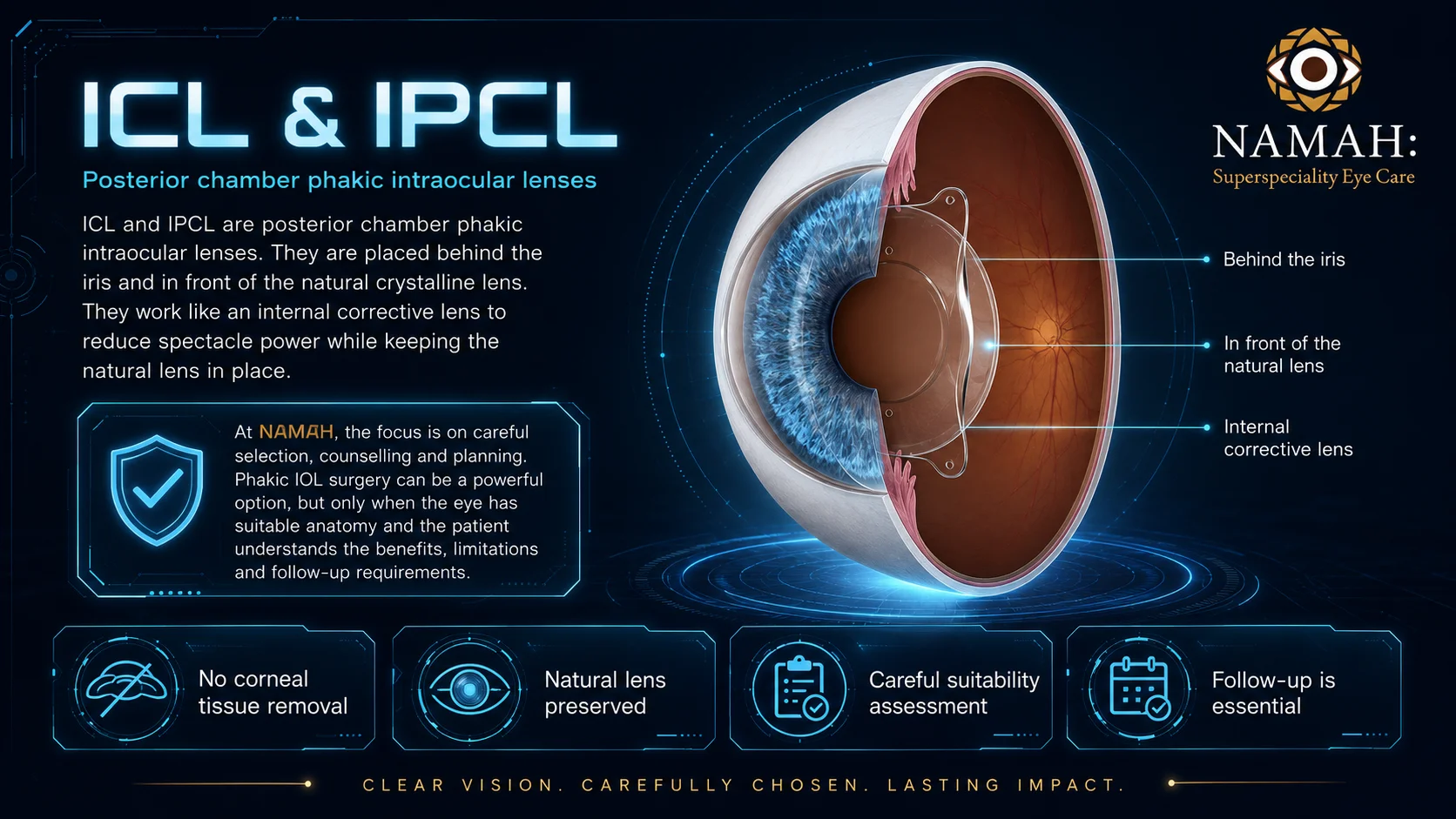
ICL & IPCL at NAMAH:
Lens-based Vision Correction for Suitable Patients
ICL and IPCL are posterior chamber phakic intraocular lenses. They are placed behind the iris and in front of the natural crystalline lens. They work like an internal corrective lens to reduce spectacle power while keeping the natural lens in place.
At NAMAH, the focus is on careful selection, counselling and planning. Phakic IOL surgery can be a powerful option, but only when the eye has suitable anatomy and the patient understands the benefits, limitations and follow-up requirements.
Potential Advantages in Properly Selected Patients
No corneal tissue remova
Useful for many patients with high myopia
Can be considered when corneal laser correction is unsuitable
Preserves the natural crystalline lens
May offer good quality of vision in properly selected patients
Can correct myopia and astigmatism depending on lens type and suitability
Important Limitations and Safety Considerations
Not suitable for every patient
Requires adequate anterior chamber depth and safe internal eye anatomy
Needs healthy cornea, retina and optic nerve
Requires accurate sizing and vault prediction
Possible risks include inflammation, raised eye pressure, cataract formation, vault-related issues, glare, halos or need for further intervention
Requires long-term follow-up
The safety and success of phakic IOL surgery depends heavily on patient selection, accurate measurements, appropriate lens sizing, surgical technique and follow-up.

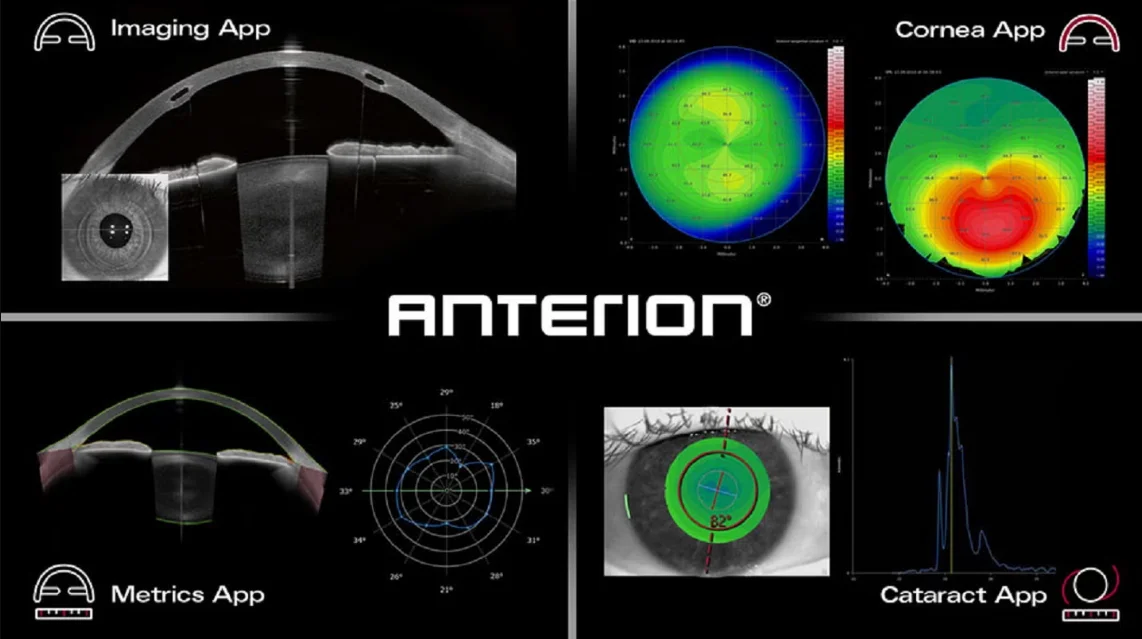
Heidelberg ANTERION:
Advanced Anterior Segment OCT for Refractive Planning
Heidelberg ANTERION is a swept-source anterior segment OCT platform used to study the front part of the eye in detail. It helps assess the cornea and the internal anterior segment anatomy that matter for refractive surgery planning.
For phakic IOL planning, the key question is not only the glasses number. Before placing an implantable lens inside the eye, we must make sure that there is enough safe space inside the eye. ANTERION helps assess this space more precisely and documents the measurements for planning and follow-up.
Potential Advantages in Properly Selected Patients
Anterior chamber depth
Corneal thickness
Corneal curvature and astigmatism
Corneal topography and tomography
Angle and anterior segment anatomy
Suitability for phakic IOL implantation
Safety planning before ICL/IPCL
Documentation for follow-up
Click on the image to zoom in
Technology does not replace surgical judgement. It improves the quality of decision-making.
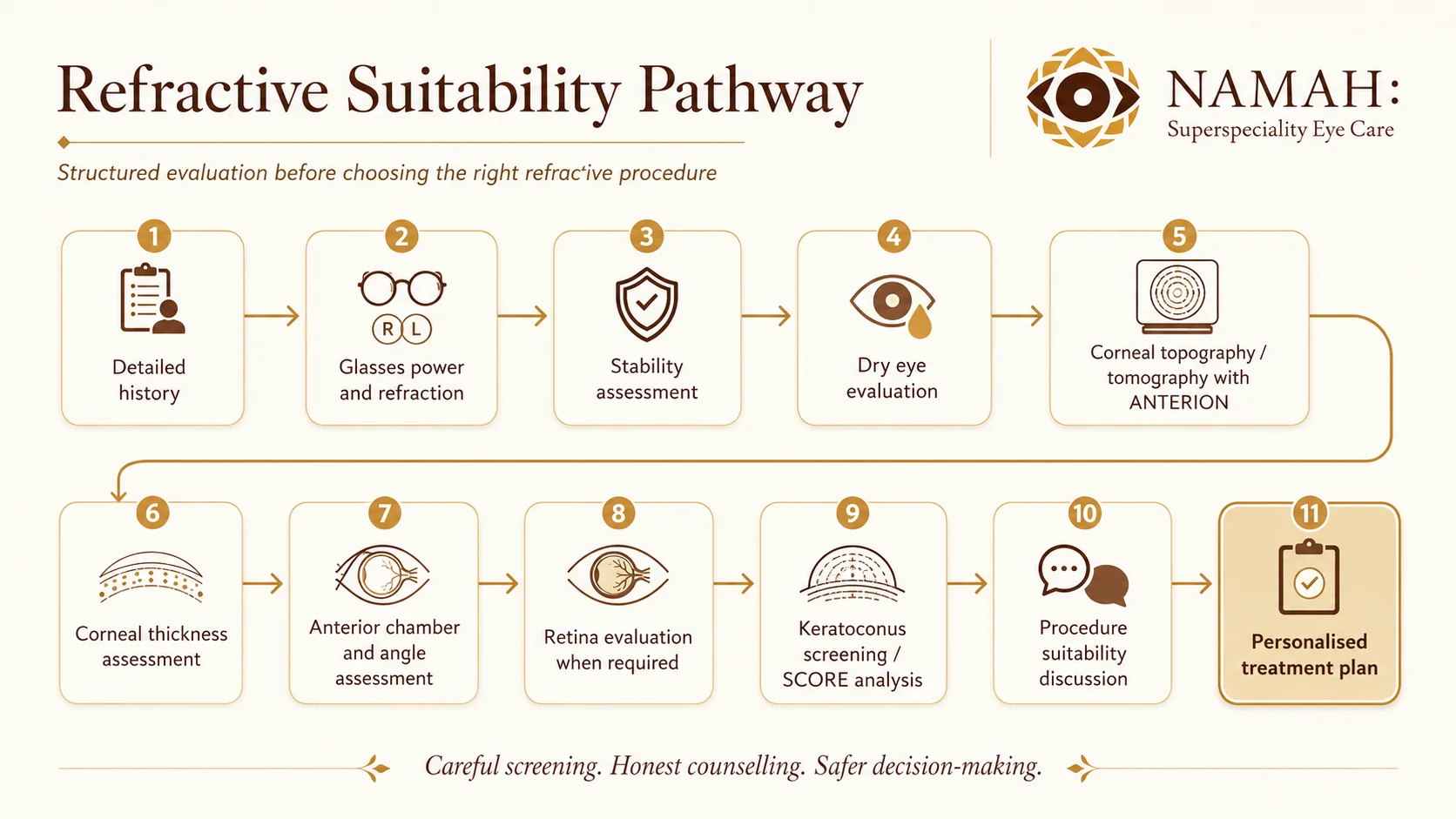
From Glasses Power to the Right Procedure
A Structured Refractive Work-up
A refractive work-up at NAMAH is designed to identify the safest and most appropriate path for each patient
The final recommendation may be:
ICL / IPCL surgery at NAMAH in suitable patients
Laser vision correction referral when appropriate
Keratoconus treatment or monitoring before any refractive decision
Dry eye treatment before refractive planning
Continuation of glasses or contact lenses
Avoiding surgery if the risk is higher than the expected benefit
Click on the image to zoom in
Click on the image to zoom in
Keratoconus Screening & Corneal Stability Assessment
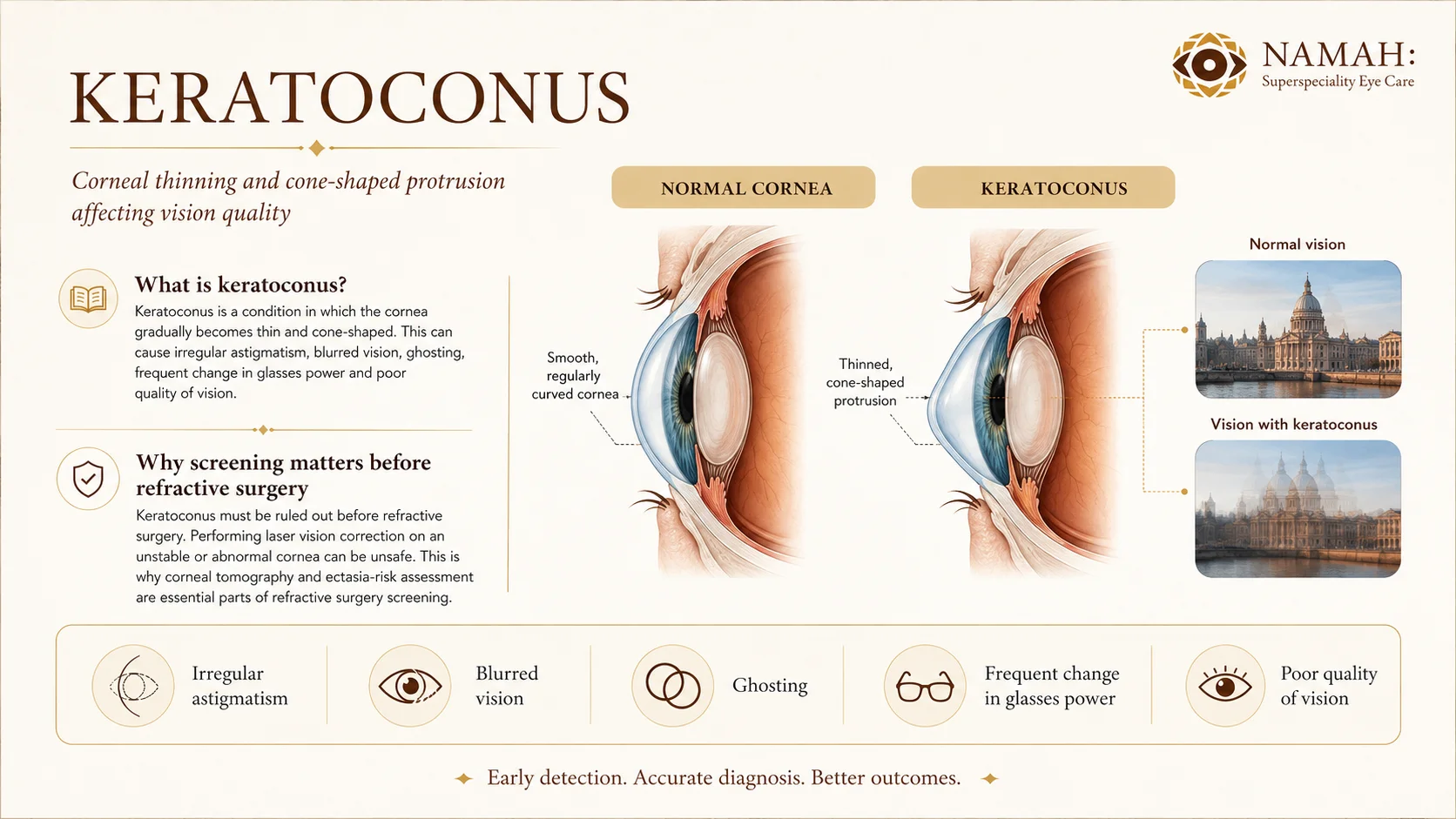
Keratoconus is a condition in which the cornea gradually becomes thin and cone-shaped. This can cause irregular astigmatism, blurred vision, ghosting, frequent change in glasses power and poor quality of vision.
Keratoconus must be ruled out before refractive surgery. Performing laser vision correction on an unstable or abnormal cornea can be unsafe. This is why corneal tomography and ectasia-risk assessment are essential parts of refractive surgery screening.
Common Signs That Need Keratoconus Evaluation
Frequent change in glasses power
Increasing cylindrical number
Poor vision despite glasses
Ghosting or double images
Eye rubbing
Allergy
Family history of keratoconus
Young patient with progressive astigmatism

Click on the image to zoom in
ANTERION SCORE
Objective Keratoconus & Ectasia-risk Screening
ANTERION provides advanced corneal imaging and ectasia-risk analysis. The SCORE system helps analyse corneal shape and tomography-based parameters to support the detection of keratoconus, suspicious corneas and ectasia risk.
SCORE does not replace clinical judgement. It supports the doctor by adding objective data to the clinical examination, refraction, corneal maps and patient history.
How SCORE-based Analysis Helps
Detecting early or suspicious keratoconus
Screening before refractive surgery
Monitoring corneal stability over time
Deciding whether laser correction is safe or unsafe
Planning keratoconus treatment such as collagen cross-linking when needed
Counselling patients realistically
Treatment Options for Keratoconus
Keratoconus treatment depends on severity, age, progression, visual quality and corneal stability. The goal is either to improve vision, stabilise the cornea, or both.
Glasses in early and mild cases
Rigid, scleral or specialty contact lenses for irregular corneas
Corneal collagen cross-linking to stabilise progression
Intracorneal ring segments in selected cases
Topography-guided treatment in selected cases at specialised centres
Corneal transplant in advanced cases

Click on the image to zoom in
At NAMAH, keratoconus care focuses on early detection, documentation, counselling and appropriate treatment planning depending on severity. Some procedures may be performed at NAMAH or coordinated through appropriate specialised centres depending on the case and technology required.
Dry Eye and Ocular Surface Before Refractive Surgery
Dry eye can affect measurements, suitability and post-operative satisfaction. A poor tear film can make vision fluctuate, affect corneal measurements and reduce the reliability of refractive planning.
Patients with significant dry eye may need ocular surface optimisation before ICL/IPCL, LASIK, SMILE or PRK planning. At NAMAH, ocular surface health can be assessed and optimised before refractive decision-making, especially in patients with screen-related dryness, contact lens intolerance or fluctuating vision.
Patient Journey for Refractive Surgery at NAMAH
Step 1
Refraction and lifestyle discussion
We understand the glasses power, visual goals, profession, screen use, night driving needs and expectations.
Step 2
Corneal and anterior segment imaging with ANTERION
The cornea and internal anterior segment anatomy are evaluated in detail for suitability and safety planning.
Step 3
Dry eye and ocular surface assessment
The tear film and ocular surface are assessed because dryness can affect both measurements and visual satisfaction.
Step 4
Keratoconus / ectasia-risk screening
Corneal stability and suspicious patterns are checked before any refractive surgery decision.
Step 5
Procedure suitability counselling
The available options are explained, including ICL, IPCL, laser referral, keratoconus care, or avoiding surgery if unsafe.
Step 6
Surgery planning, referral or follow-up decision
A personalised plan is made based on safety, suitability, lifestyle and realistic expected outcomes.
Frequently Asked Questions
Which is better - LASIK, SMILE, PRK, ICL or IPCL?
There is no single best procedure for everyone. The right option depends on power, corneal thickness, corneal shape, dry eye status, anterior chamber depth, retina health and lifestyle needs.
Does NAMAH perform LASIK or SMILE?
NAMAH currently focuses on refractive evaluation, suitability assessment and phakic IOL surgery such as ICL/IPCL in suitable patients. LASIK, SMILE and PRK are explained for education and may be advised at a specialised laser refractive centre when appropriate.
What is ICL?
ICL is an implantable phakic intraocular lens placed inside the eye while preserving the natural crystalline lens. It helps correct spectacle power without removing corneal tissue.
What is IPCL?
IPCL is another type of phakic intraocular lens used for selected patients. Like ICL, it is placed inside the eye and requires careful measurement, sizing and follow-up.
Who is suitable for phakic IOL surgery?
Suitability depends on stable power, adequate anterior chamber depth, healthy cornea, normal retina and optic nerve, appropriate age and realistic expectations.
Is ICL/IPCL better for high myopia?
Phakic IOLs are often useful in selected high myopia patients, especially when laser correction is unsuitable. However, final suitability depends on detailed measurements and eye health.
Is phakic IOL surgery reversible?
Phakic IOLs can usually be removed if required, but this does not make the procedure risk-free. It is still an intraocular surgery and requires proper counselling and follow-up.
Can ICL/IPCL correct astigmatism?
In selected patients, toric phakic IOL options may help correct astigmatism. Suitability depends on the amount and pattern of astigmatism and lens availability.
Why is ANTERION needed before refractive surgery?
ANTERION helps assess corneal shape, thickness, anterior chamber depth and other anterior segment parameters. These measurements support safer decision-making, especially for ICL/IPCL and keratoconus screening.
Why is keratoconus screening important before LASIK?
Keratoconus or suspicious corneal weakness can make laser vision correction unsafe. Screening helps identify patients who should avoid laser surgery or need corneal treatment first.
What is the ANTERION SCORE system?
The SCORE system is an ectasia-risk analysis tool that supports keratoconus and suspicious cornea detection using tomography-based parameters. It supports, but does not replace, clinical judgement.
What happens if I am not suitable for refractive surgery?
You will be counselled honestly. The recommendation may be glasses, contact lenses, dry eye treatment, keratoconus monitoring or treatment, laser referral, ICL/IPCL, or avoiding surgery if it is not safe.
At NAMAH, refractive vision correction is built on careful screening, advanced anterior segment imaging, honest counselling and personalised treatment planning. Whether the right option is ICL, IPCL, laser vision correction referral, keratoconus monitoring, corneal treatment or avoiding surgery altogether, our aim is to guide every patient towards the safest and most appropriate decision for their eyes.